
Injury Recovery: Safe Return to Play
You felt the injury the moment it happened. Maybe it was a sharp grab in the knee cutting sideways for a ball, a shoulder that didn’t feel right after a lift, or a head impact that left you foggy later that day. The first question is almost always the same. How long until I can get back?
That question makes sense. Activity is part of how many people manage stress, stay social, and feel like themselves. When that routine disappears, frustration shows up fast. I see it in competitive athletes, adult league players, runners, and people who just want to get back to the gym without second-guessing every movement.
The problem is that fast and ready are not the same thing. A calendar can tell you how much time has passed. It can’t tell you whether your knee can absorb force, whether your shoulder can control speed overhead, or whether your brain has recovered enough for contact, reaction, and decision-making. That’s where return to play matters. It gives you a roadmap when emotion, pressure, and guesswork start pulling you off course.
The Frustration of the Sideline and the Path Back
A common scene in clinic looks like this. Someone limps in a few days after an injury and says, “It already feels better. I just need to know when I can test it.” That’s an honest reaction, but it’s also where setbacks begin. Early improvement can be misleading. Pain often settles before strength returns. Swelling can calm down before movement quality is restored. Confidence can come back before the tissue is fully ready for sport demands.

Why impatience is so common
For active people, being sidelined isn’t just inconvenient. It can feel like losing part of your routine and identity. That’s why people rush. They don’t want to miss games, training progress, social connection, or momentum. If you’ve been injured, that urgency probably feels familiar.
What helps is a shift in the question:
- Instead of asking how fast can I return, ask what your body has to prove before it’s safe.
- Instead of chasing pain-free movement alone, focus on force, control, endurance, reaction, and confidence.
- Instead of treating rehab like a waiting room, treat it like training with checkpoints.
Return to play isn’t a wall between you and your sport. It’s the safest route back to doing it well.
Some people find it helpful to hear broader conversations about healing, tissue recovery, and why shortcuts often backfire. If that’s useful to you, the Peak Performance podcast offers a longer discussion on recovering the right way instead of just chasing a quick return.
The better goal
The primary target isn’t getting back for one practice. It’s getting back and staying back. That means returning with enough capacity to tolerate training, enough coordination to move efficiently, and enough trust in your body to compete without guarding every step.
When people understand that, the process feels less like a delay and more like a plan.
What Return to Play Really Means
Return to play is often misunderstood as a date on the calendar. It isn’t. In practice, it’s a medically supervised progression where each step depends on whether the athlete meets specific criteria.
Definition: Return to play is a criteria-based medical process, not a simple countdown. You move forward when you demonstrate recovery, not when enough days have passed.
That difference matters because tissues, joints, and the nervous system don’t all recover on the same schedule. Two people can have the same diagnosis and look very different in rehab. One may have pain under control but poor balance. Another may be strong in a clinic setting but struggle when speed, fatigue, and quick decisions are added.
Time-based recovery versus criteria-based recovery
A time-based model says, “It’s been long enough.”
A criteria-based model asks harder and better questions:
| Approach | What it relies on | Main limitation |
|---|---|---|
| Time-based | Calendar milestones | Can miss weakness, instability, poor movement quality, or lingering symptoms |
| Criteria-based | Function, symptoms, testing, progression tolerance | Takes more discipline and more objective follow-up |
The criteria-based approach is safer because sport is not a basic daily activity. It combines impact, force, speed, reaction, fatigue, and unpredictability. A body part may tolerate walking and still fail under cutting, landing, sprinting, overhead loading, or contact.
Who makes the decision
A good return to play decision is shared. The patient matters because symptoms, confidence, and goals matter. The therapist matters because movement quality, strength, and progression need to be tested. The physician matters when diagnosis, healing status, imaging, medication, or medical clearance are part of the picture.
That team process protects you from two common mistakes:
- Returning because pain is lower
- Returning because an important date is coming up
If your recovery plan has no objective checkpoints, it’s not really a return to play plan. It’s hope with a deadline.
The Staged Return to Play Protocol Explained
The clearest model for understanding return to play is the graduated concussion progression. Even if your injury isn’t a concussion, the logic applies broadly. You don’t jump from rest to full competition. You move through stages that stress the body and brain a little more each time, and you only advance if you tolerate the stage well.
The standard progression uses a 24-hour symptom-free rule. Athletes must recover to baseline across multiple areas before moving forward, including cognitive function, vestibular stability, sensorimotor response, and behavioral normalization, according to the Brain Injury Association of America guidance on return to play.
How staged progression works
Think of this like rebuilding a bridge after damage. You don’t open it to full traffic because the surface looks repaired. You test whether it can handle light load, then heavier load, then speed and repetition.
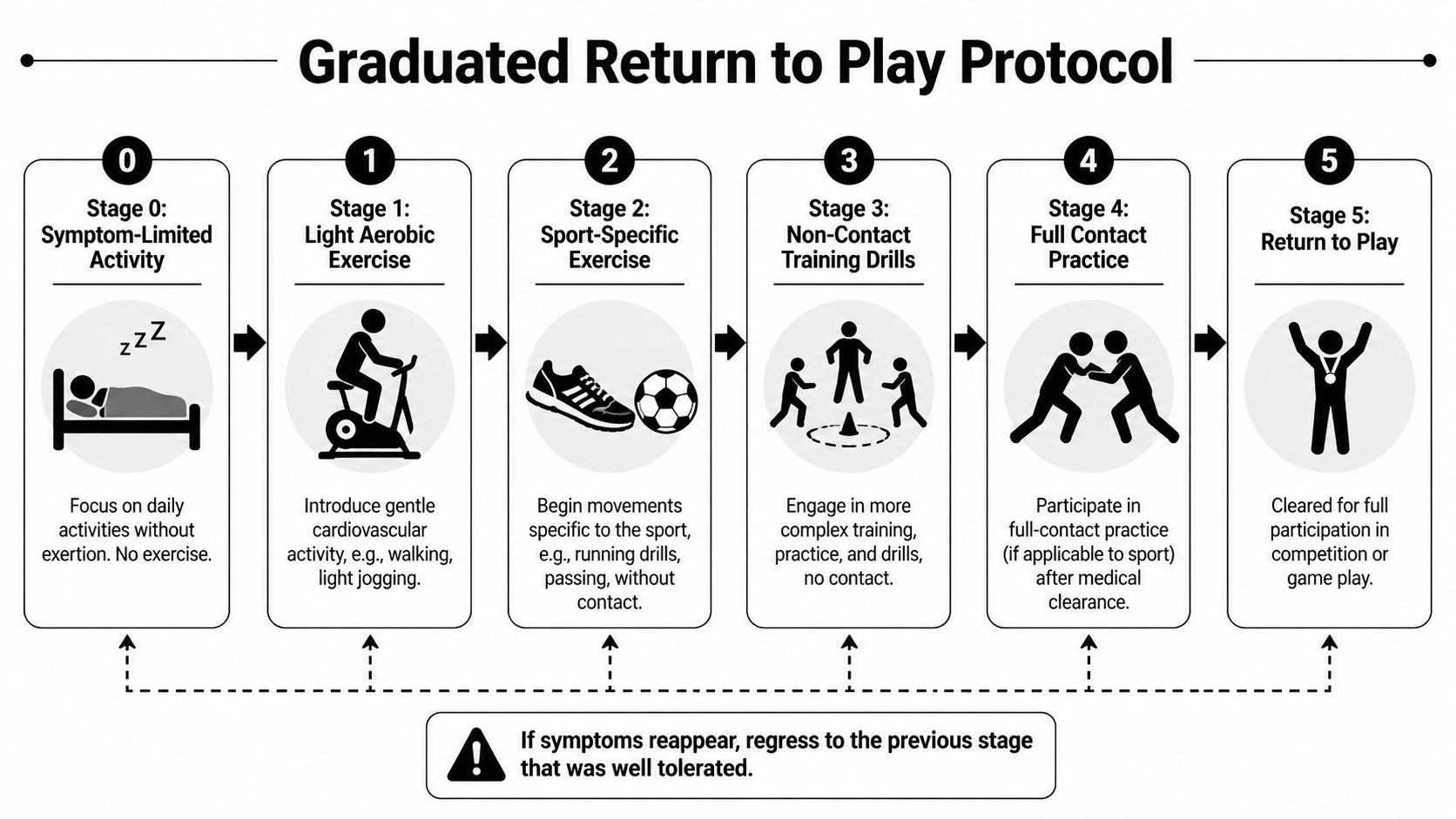
A practical progression often looks like this:
Symptom-limited activity
Daily activity is allowed within tolerance, but not exercise that provokes symptoms.Light aerobic work
Walking, easy cycling, or other controlled cardiovascular work begins.Sport-specific movement
Running patterns, footwork, passing patterns, or controlled skill work can start without contact.Non-contact training drills
More complex movement and reaction are added. The athlete has to tolerate higher speed and more decision-making.Full-contact practice after clearance
This is not the first testing day. It happens after prior stages are passed.Return to play
Full participation resumes.
The rule most people need to hear
If symptoms return, you don’t push through and “see if it settles.” You go back to the previous stage. That isn’t failure. It’s the protocol doing its job.
For concussion care, objective tools matter. The Post-Concussion Sway test is one example specifically highlighted as a validated balance assessment that should return to pre-injury baseline before progression begins in that framework. That’s what criteria-based rehab looks like in real life. You measure what matters.
There’s also good reason to respect structured rehab beyond concussion. An integrated on-field rehabilitation framework in professional football reduced total player absence days from 1,162 in the 2022 to 2023 season to 468 in 2024 to 2025, lowered lost days per 1,000 hours of training exposure from 100 to 29.5, and reduced average return-to-play time by about 7 days, as reported in this sports medicine review of advanced return-to-play frameworks. That same source notes that reliance on timeframes and subjective assessment alone leaves athletes exposed, including a 38% hamstring re-injury rate within six months in footballers under those weaker models.
If you’re working through a sports injury, this is the standard to aim for: staged progress, objective testing, and sport-specific decisions. That’s also the philosophy behind physical therapy for sports injuries, where rehab has to prepare the athlete for actual demands, not just basic daily tasks.
Timelines and Tests for Common Sports Injuries
People understandably want timelines. The problem is that timelines are averages, not permission slips. They’re useful for setting expectations, but they should never replace testing.

What a timeline can and can’t tell you
For some injuries, we do have concrete published data. In major American sports leagues, professional athletes with patellar fractures had a 71% return-to-play rate with an average recovery timeline of 217 days, based on a study of athletes from the NFL, NBA, MLB, and NHL in the patellar fracture return-to-play study on PubMed. The same study found an important pattern. Athletes treated operatively showed an initial performance drop in year 1 compared with matched controls, but recovered to similar performance by year 2, while nonoperative athletes showed continued decline in year 2.
That’s useful, but it doesn’t mean day 217 is your green light. It means recovery often takes longer than people hope, and durable performance usually depends on what happens after pain settles.
Common examples in clinic
For orthopedic injuries, I explain clearance in terms of demands, not just diagnosis.
Knee injuries need more than full range of motion. The athlete has to control landing, deceleration, cutting, and single-leg loading. Common tests may include single-leg squat quality, hop testing, and side-to-side strength comparison.
Shoulder injuries have to prove control at speed. Being able to raise the arm overhead in the clinic is not the same as throwing, swimming, serving, or lifting under fatigue. We look at strength, endurance, scapular control, and whether symptoms return with repeated effort.
Ankle sprains often fool people. Walking comes back early, but quick direction changes, uneven surfaces, and reactive balance expose lingering deficits. Balance testing, calf strength, hopping tolerance, and confidence matter.
A useful rehab test answers this question: can you handle the next demand without compensation, symptom flare, or loss of control?
Patients also ask when imaging is needed. Pain location, trauma history, swelling, locking, weakness, and failed progression can all change that decision. If you’re trying to sort through that question, this guide on when you need an MRI and when you need an X-ray can help frame the discussion with your medical team.
A quick visual walkthrough can also make the rehab progression easier to understand:
The trade-off that matters
Returning too early may let you participate sooner. It may also reduce how well you move, how confidently you perform, and how long you stay available. In other words, the shortest route back to activity can be the longest route back to your real level.
Critical Safety Checks and Red Flags
A safe return to play plan needs brakes, not just a gas pedal. Patients usually understand this once they’ve had one setback. The hard part is recognizing red flags early enough to avoid that setback in the first place.

Physical signs that mean stop
The body usually gives you useful information if you listen to the right signals.
- Pain that escalates during or after activity means the load may be too high.
- Swelling that returns suggests the joint or tissue is not tolerating progression.
- Instability, buckling, or giving way is never something to train through.
- Loss of motion after activity often means irritation exceeded capacity.
- Compensated movement such as limping, trunk leaning, guarding, or altered arm mechanics tells you the body is finding workarounds instead of performing normally.
Those signs don’t automatically mean severe damage. They do mean the current stage may be too advanced.
Cognitive and behavioral red flags
With concussion or any injury involving high stakes, mental pressure can distort judgment. Fogginess, dizziness, poor balance, slowed reaction, confusion, symptom recurrence, or feeling “off” all deserve caution. The Brain Injury Association guidance states that recurrence of symptoms means the person has not fully recovered within that progression model. That should be taken seriously.
There’s also a less obvious red flag. Impatience itself. The athlete who keeps saying “I’m fine” before testing is completed may be responding more to urgency than readiness.
Slowing down at the right moment often protects the fastest complete recovery.
Professional sports have recognized that pressure can cloud medical decisions. The NFL requires players to complete a five-step process through team medical staff and then receive final clearance from an independent neurological consultant, as detailed in the NFL concussion return-to-participation protocol. That dual-verification model is a useful lesson for everyone, not just pros. High-stakes returns need objective gatekeepers.
For athletes and active adults thinking beyond one season, prevention belongs in the same conversation as recovery. Resources that discuss how to optimise athletic longevity can be useful once you’re rebuilding training habits after injury.
How MedAmerica Supports Your Safe Return in Deerfield Beach
A durable return to play usually requires more than one lens. The injured area matters, but so do movement mechanics, pain control, loading strategy, confidence, and the patient’s ability to stay consistent when progress feels slow.
What a multidisciplinary plan looks like
At sports therapy, MedAmerica Rehab Center can support return to play through a multidisciplinary model that may include physical therapy, chiropractic care, acupuncture, and progressive exercise. Each piece has a different role.
Physical therapy handles the progression. That includes restoring strength, mobility, balance, and sport-specific movement, then using functional testing to decide whether the next stage is appropriate. Here, criteria-based rehab becomes practical instead of theoretical.
Chiropractic care can help address joint and movement restrictions that change how force travels through the body. That matters when someone starts compensating around an injury and loads the wrong area.
Acupuncture may help with pain modulation and symptom management, especially when discomfort is interfering with sleep, exercise tolerance, or training consistency. It doesn’t replace rehab, but it can make rehab easier to perform well.
Treating the whole person
One of the biggest reasons people derail recovery isn’t pain. It’s frustration. Northwestern Medicine notes that many athletes are “overly eager to return to sports” and that a patient-centered approach should address motivation, confidence-building, and the mental strain of prolonged rehabilitation in its discussion of what return to play really means.
That point matters in everyday practice. A patient may be physically improving but mentally done with the process. They start skipping home exercises, testing themselves outside the plan, or chasing workouts that feel familiar instead of doing the ones that move recovery forward.
A multidisciplinary team can respond to that in concrete ways:
- By breaking rehab into visible wins so progress feels real before full sport is allowed.
- By using progressive drills that rebuild trust, starting with controlled movement and adding complexity only when earned.
- By coaching expectations clearly so the patient knows why a stage is being held or advanced.
- By treating setbacks as data instead of as failure.
Confidence should be rebuilt the same way strength is rebuilt. Progressively, objectively, and with enough repetition that it holds up under stress.
That whole-person approach is what makes return to play durable. You’re not just calming symptoms. You’re preparing a person to handle the physical and psychological demands of getting back out there.
Your Recovery Is a Journey Not a Race
The safest return to play plan rarely feels like the fastest one in the moment. It asks you to respect stages, pass tests, and hold back when emotion tells you to push. That can be frustrating, especially when you miss training, competition, or the routines that keep you grounded.
It’s still the right approach.
The takeaways that matter most
- Time matters, but it doesn’t decide readiness by itself.
- Criteria-based progression protects you better than guesswork.
- Symptoms, strength, balance, movement quality, and confidence all count.
- Regression is part of smart rehab when the body says a stage was too much.
- The goal is not a quick appearance. The goal is a stable return.
If you’re recovering from a sports injury, surgery, concussion, or recurring setback, don’t judge your progress by whether you can survive one workout. Judge it by whether your body can repeat demands safely and consistently.
A good return to play process does more than get you back. It builds a stronger foundation under the movement that matters to you, whether that’s league play, weekend tennis, lifting, running, pickleball, or trusting your body again.
If you’re in Deerfield Beach or a nearby community and want a structured plan for getting back to sport or activity safely, schedule a consultation with MedAmerica Rehab Center. A personalized return to play plan can help you move past guesswork, understand your real checkpoints, and return with more confidence in your body and your long-term health.