
One to One Therapy for Lasting Pain & Injury Recovery
You might be dealing with this right now. Your back hurts, your knee still doesn’t trust stairs, or your shoulder never felt the same after an accident. You finally commit to therapy, show up hopeful, and end up in a busy gym where one clinician is bouncing between several people. You get a sheet of exercises, a few quick cues, and a sense that your body has been folded into a standard routine.
That model can work for some people. It often falls short when pain is stubborn, movement is compensating, or recovery needs careful progression.
In physical rehabilitation, one to one therapy means something simple and important. Your session is built around your body, your pain pattern, your goals, and your response that day. If your sciatica flares during a movement, the plan changes. If your balance drops after surgery, the therapist adjusts on the spot. If your neck pain is really coming from how your shoulder blade moves, someone catches it before you spend weeks doing the wrong thing.
That’s the difference many patients are looking for. Not more activity. Better attention.
Beyond the Crowded Waiting Room
A lot of patients arrive after trying a version of rehab that felt impersonal. They were told to stretch, strengthen, and keep moving, but nobody spent enough time figuring out why one exercise helped while another made things worse. They weren’t lazy or noncompliant. They just didn’t get enough skilled attention.
That matters in physical therapy because pain rarely behaves like a checklist. A person with low back pain may also have hip stiffness, poor trunk control, and a walking pattern that keeps loading the same irritated area. Another person with the same diagnosis may need a completely different approach because the main driver is weakness after surgery, a balance problem, or fear of movement after an auto accident.
When generic rehab misses the point
In a crowded setting, the small details often get missed:
- Form drift: Your squat starts well, then your weight shifts, your knee caves in, or your back takes over.
- Pain behavior: A movement might be fine for five reps, then symptoms begin traveling, tightening, or burning.
- Pacing mistakes: Some people need more challenge. Others need less load and better control first.
- Compensation patterns: The body is great at finding workarounds. Those workarounds often become the next injury.
Practical rule: If therapy feels like you're teaching yourself while someone checks in from across the room, you're probably not getting the level of physical rehabilitation your body needs.
One to one therapy is the opposite of that experience. It puts a licensed therapist with one patient for the session, with enough time to assess movement, use hands-on treatment when needed, and coach each exercise so it transfers to daily life. For someone with sciatica, arthritis, post-surgical stiffness, or dizziness during walking, that focused setup can make rehab feel clearer and safer.
In Deerfield Beach, that approach matters for practical reasons too. People want pain relief, but they also want to drive comfortably, sleep through the night, get back to work, walk without fear, and stop worrying that every flare means something is going backward.
What Is One to One Physical Therapy
Think of it as the difference between a private tutor and a large lecture hall. In the lecture hall, you hear the material, but the pace and the message are built for the room. With a private tutor, every minute responds to what you understand, where you struggle, and what needs correction.
That’s what one to one physical therapy looks like in practice.

What happens during the session
In this model, the therapist provides undivided attention for the full session, which typically lasts 45 to 60 minutes, allowing real-time movement analysis and on-the-spot adjustments. Outpatient clinics built to support this level of care typically schedule therapists to see 8 to 12 patients per day, which leaves room for treatment and documentation without rushing, according to Platinum Physical Therapy's overview of one-on-one care.
That time changes the quality of care. The therapist can watch how you sit down, stand up, turn, reach, walk, and load a painful joint. They can test whether your pain is coming from stiffness, weakness, nerve irritation, poor motor control, or a combination of several factors. Then they can treat the problem in front of them, not the diagnosis on the intake form.
A true one to one session usually includes a mix of:
- Hands-on treatment: Manual techniques such as soft tissue work, joint mobilization, or guided movement when appropriate.
- Targeted exercise: Not a generic printout, but movements selected for your limitations and goals.
- Immediate correction: If your posture, gait, or mechanics drift, the therapist catches it right away.
- Education: You learn what the pain likely means, what to avoid for now, and what to keep doing.
It’s a dynamic process, not a canned routine
The plan should change as your body changes. Some days you’re ready to progress. Other days swelling, fatigue, or a pain flare means the therapist needs to pivot. That flexibility is one of the biggest strengths of one to one therapy.
If you want a clearer picture of what that visit feels like from check-in through treatment, this guide to what a typical physical therapy session looks like is useful before your first appointment.
For people who need broader symptom support alongside rehabilitation, it can also help to understand other effective pain relief options that may complement a structured therapy plan.
A good session doesn't just make you tired. It tells you something useful about your body.
The Transformative Benefits of a Personalized Approach
Personalized rehab works because it removes guesswork. Instead of asking, “Did that exercise bother you?” after the fact, the therapist sees what happened, adjusts the angle, changes the load, or swaps the movement entirely. That’s how progress becomes more consistent.
Research summarized by Beaming Health's therapy statistics review reports that 75 to 80% of patients experience meaningful benefits from one-to-one therapy, and 50% of clients show improvement after just 8 sessions. In physical rehabilitation, that kind of focused attention often shows up as cleaner movement, lower pain during everyday tasks, and fewer setbacks from doing too much too soon.

Faster progress because the plan fits the person
A post-surgical knee doesn’t need the same progression as a long-standing arthritic knee. A runner with hip pain doesn’t need the same cues as a senior working on balance. One to one therapy allows the therapist to dose treatment precisely.
That can mean:
- backing off a movement before it aggravates a healing joint
- progressing resistance once control improves
- changing a walking drill because your ankle, not your knee, is limiting stride
- spotting that your low back pain shows up most when rotation and fatigue combine
When treatment fits the problem, patients usually waste less time on exercises that don’t move the needle.
Better movement means lower re-injury risk
Pain relief matters, but it isn’t enough by itself. If you still bend, walk, lift, or reach with the same faulty mechanics, symptoms often return.
Movement retraining becomes essential. A therapist might notice that your pelvis shifts during a step-up, that your shoulder hikes during overhead motion, or that your foot collapses during single-leg work. Correcting those patterns can change how force travels through the body. That’s one reason many programs include neuromuscular reeducation, which helps rebuild better control and coordination.
The body doesn't always choose the healthiest movement. It chooses the movement it can manage. Therapy should teach it a better option.
Plateaus usually need precision, not more effort
Many people hit a plateau because they keep adding effort to the wrong strategy. More stretching won’t fix a stability problem. More strengthening won’t help if pain spikes because the movement pattern is off.
One to one therapy helps break those stalls by narrowing in on the limiting factor. Sometimes that’s joint mobility. Sometimes it’s timing, balance, fear of loading, or poor trunk control after an injury. Active adults who want to bridge rehab into performance often benefit from seeing how that same individualized thinking carries into personalized training programs, where movement quality still drives the plan.
The result patients usually notice first isn’t dramatic. It’s practical. They get out of bed with less guarding. They walk farther before symptoms start. They trust stairs again. That’s what lasting recovery tends to look like.
One to One Therapy Compared to Group Sessions
Group sessions have a place. They can create accountability, lower the pressure some patients feel when starting, and offer social support. For straightforward conditioning, general mobility work, or maintenance exercise, that environment can be helpful.
But group care and one to one therapy are not interchangeable. If you need manual therapy, close symptom monitoring, gait correction, balance challenge, or post-operative progression, divided attention becomes a real limitation.
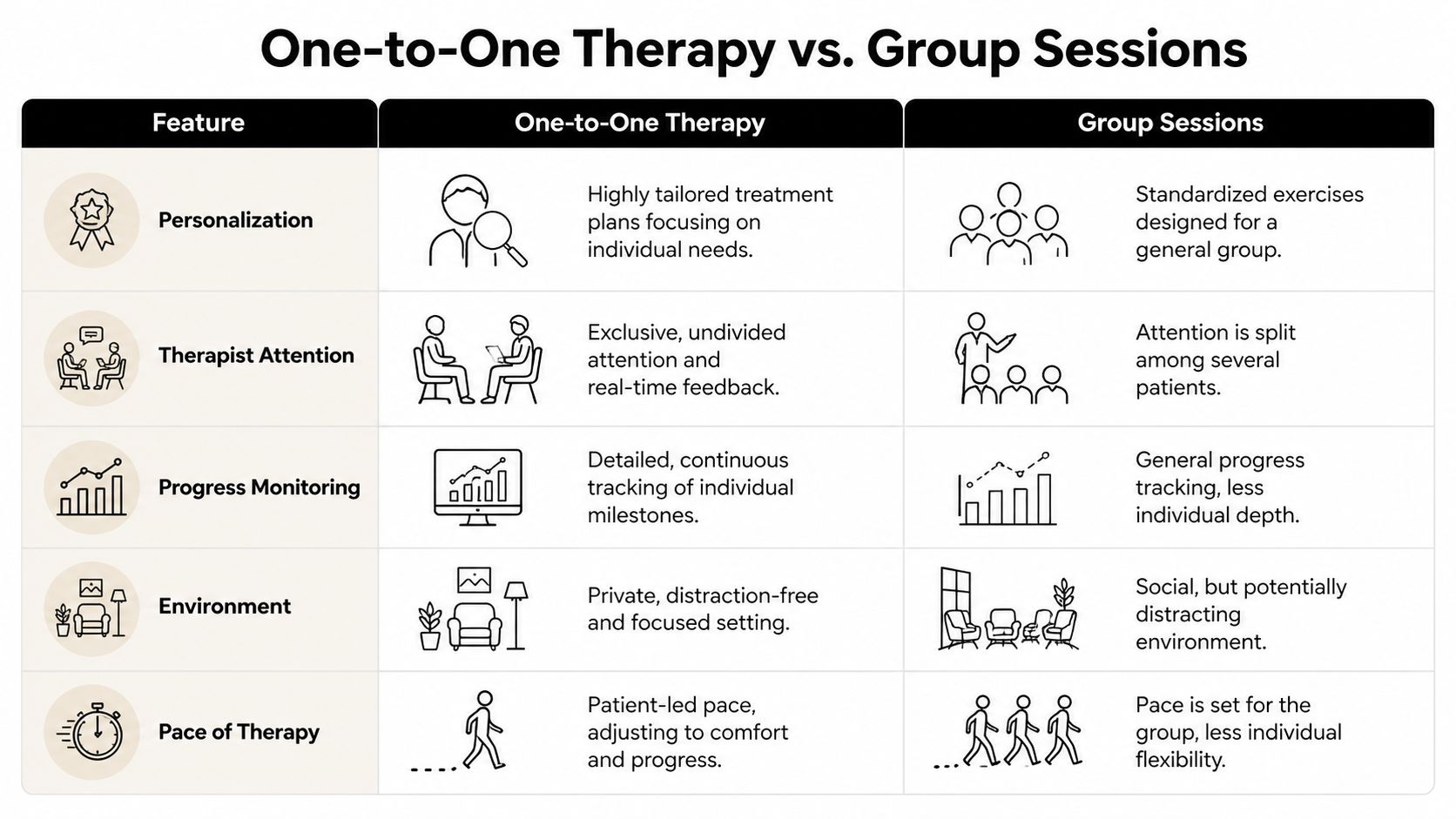
One to One Therapy vs. Group Therapy at a Glance
| Feature | One to One Therapy | Group Therapy |
|---|---|---|
| Personalization | Treatment is tailored to your symptoms, movement limits, and goals | Exercises are usually broader and designed to fit several people |
| Therapist attention | One patient has the therapist’s focus during the session | Attention is split across the room |
| Progress monitoring | Small changes are easier to catch and address right away | Progress is monitored more generally |
| Environment | Quieter and more private | More social, but also more distracting |
| Pace of therapy | The session can slow down or progress based on your response | The pace often has to fit the group |
The biggest difference is feedback
The therapeutic relationship in one-to-one sessions accounts for up to 30% of treatment outcomes, and that close partnership supports continuous coaching and real-time feedback, according to this review in the National Center for Biotechnology Information archive. In physical rehab, that translates into something concrete. Someone is watching whether your symptoms centralize or spread, whether fatigue changes your mechanics, and whether your confidence drops when a task gets harder.
That’s difficult to reproduce in a group setting.
For example, someone recovering from sciatica may need repeated changes in position, tempo, and exercise selection during a single visit. A patient working on fall prevention may look steady at first, then lose control once head turns or uneven surfaces are added. A person after shoulder surgery may need hands-on guidance to protect healing tissue while restoring range. Those decisions depend on close observation.
When group sessions can still make sense
Group therapy isn’t “bad.” It’s just better suited to certain situations.
- General conditioning: Useful when the goal is broad exercise tolerance.
- Maintenance phase: Helpful after the skilled rehab phase is complete.
- Motivation: Some people enjoy the social energy and routine.
- Lower complexity: Simpler cases may not need constant adaptation.
If your condition changes rep to rep, you need a setting that can change rep to rep with it.
For pain, injury, and mobility problems that require precise progression, one to one therapy gives the therapist more chances to make the right decision at the right moment.
Your Recovery Journey Step by Step
Starting therapy feels easier when you know what will happen. Most patients don’t need more medical jargon. They need a clear sense of what the first visit looks like, what a normal session includes, and how progress gets measured.

The first visit
The first session should begin with listening. Not just “Where does it hurt?” but questions that reveal the pattern.
When did it start? What brings it on? What eases it? Do symptoms travel? Are mornings worse? Are you avoiding stairs, driving, lifting, sleeping on one side, or walking certain distances? Those details matter because they often tell us more than the pain rating alone.
After that comes the physical assessment. Depending on the issue, the therapist may examine range of motion, strength, swelling, walking mechanics, balance, joint mobility, and how specific movements affect symptoms.
A good first visit usually ends with three things:
- A working explanation of what seems to be driving the problem.
- A treatment direction that makes sense for your body today.
- A home plan that is realistic enough to follow.
What a treatment session feels like
Most one to one sessions blend several tools rather than relying on one method. A patient with back pain might start with mobility work, move into trunk control drills, then practice hip hinging with careful cueing. Someone recovering from a knee injury might work on swelling management, range of motion, quadriceps activation, and walking mechanics in the same visit.
The key is that the therapist is watching the whole time. If pain climbs, the dosage changes. If control improves, the task progresses. If fatigue creates bad form, the exercise gets simplified before it reinforces a compensation.
Common elements include:
- Manual therapy when indicated: Used to improve mobility, reduce guarding, or help a stiff area move more normally.
- Corrective exercise: Chosen to restore strength, control, endurance, and confidence.
- Functional practice: Sit-to-stand, stairs, reaching, lifting, turning, or gait tasks that match real life.
- Education: Clear advice on pacing, posture, flare management, and what to do between visits.
How progress gets tracked
Progress is more than “it hurts less.” We look for changes that matter in daily life. Can you roll in bed with less pain? Walk through the grocery store without stopping? Reach overhead without shrugging? Get up from a chair without using your hands?
Some gains are objective. Range improves. Balance gets steadier. Walking becomes more symmetrical. Some gains are personal. You return to pickleball, drive without fear, or pick up a grandchild again.
Recovery isn't linear. What matters is whether the trend is moving toward better function, better tolerance, and better control.
Outside the clinic, simple habits support the work. Sleep, pacing, hydration, and nutrition all affect tissue recovery. For patients who want practical nutrition support, Gym Snack's complete guide to recovery foods is a useful starting point.
The MedAmerica Rehab Center Difference
A one to one model works best when the clinic around it supports consistent care. That means enough scheduling flexibility for follow-up visits, help with insurance questions, and a team that can coordinate when pain overlaps with more than one issue.
For many patients, recovery isn’t just one lane. A person might need physical therapy for movement restoration, chiropractic care for joint restrictions, acupuncture for pain modulation, or guided balance training after a fall. When those services live under one roof, treatment decisions can stay connected instead of fragmented.
Why access matters as much as technique
Consistency is a major part of good outcomes. Data summarized in the earlier research shows that clinics where patients attend an average of 1.83 visits per week can reach successful discharge rates as high as 93%, highlighting how much regular one-to-one care matters in physical rehabilitation. If scheduling is difficult or communication is poor, even a strong treatment plan can lose momentum.
That’s why practical details matter:
- Same-day availability: Helpful when pain spikes, a new injury happens, or a recent surgery needs quick follow-up.
- Insurance guidance: Important for auto accident and workers’ compensation cases, where paperwork can slow care if nobody helps.
- Multidisciplinary coordination: Useful when symptoms involve pain, stiffness, weakness, and recovery anxiety at the same time.
Patients who want to know who may be involved in their care can review the clinic team and treatment disciplines.
What that looks like in real life
At MedAmerica Rehab Center, patients can receive individualized rehabilitation for back pain, sciatica, arthritis, post-surgical recovery, sports injuries, and accident-related conditions, with access to physical therapy, chiropractic care, acupuncture, and other non-surgical options in one setting.
That combination doesn’t replace skilled one to one therapy. It supports it. When care is coordinated well, patients spend less time repeating their story and more time moving forward.
Common Questions About Starting Therapy
People usually ask practical questions first. That makes sense. You want to know whether therapy fits your schedule, whether insurance will help, and whether the process will be manageable if you're already in pain.
Is one to one therapy covered by insurance
Coverage depends on your plan and the reason for treatment. For many patients, especially after auto accidents or work injuries, one-to-one physical therapy may be covered through insurance arrangements tied to those cases. Affordability is a real barrier, with 42% of Americans citing cost as a major obstacle to care, and insurance-friendly clinics can help patients work through their options, according to Open Path Collective's affordability resource.
If you’re unsure, ask the clinic to verify benefits before the first visit and explain any authorizations, visit limits, or accident-related documentation.
How many sessions will I need
That depends on the condition, severity, irritability, and how consistently you attend and follow the plan between visits. A fresh ankle sprain often moves differently than chronic neck pain, post-operative stiffness, or long-standing sciatica.
A reliable clinic should give you a working estimate after the evaluation, then update that estimate based on how you respond. If nobody is reassessing your progress, that’s a concern.
Will therapy hurt
Some discomfort is normal. Sharp escalation, lasting aggravation, or feeling worse for days after every session is not a good sign. One to one therapy helps here because the therapist can adjust in real time instead of realizing later that the session overshot your tolerance.
Do I need a referral
That depends on your insurance and the type of case. Some plans allow direct access, while others require a referral or authorization. Workers’ compensation and auto accident cases often have their own documentation rules.
What should I bring to the first appointment
Bring any imaging reports you have, a medication list if relevant, your insurance information, and shoes or clothing you can move in. If walking, balance, or stairs are part of the problem, mention that early so the evaluation includes those tasks.
How do I know if a clinic really offers one to one therapy
Ask directly who stays with you during the session. Ask whether a licensed therapist treats you for the full visit, whether manual therapy and exercise are both available, and whether your program changes based on your response that day. Clear answers matter.
If you’re dealing with pain, stiffness, injury recovery, or balance problems and want care built around your body rather than a busy room, MedAmerica Rehab Center is one place to start. Ask about the first visit, insurance questions, and whether one to one therapy is the right fit for your condition and goals.