Pain Neuroscience Education a New Approach to Pain Relief
Most pain advice starts with a simple message: if it hurts, something must be damaged.
That idea makes sense for a fresh injury. If you sprain an ankle, your body needs protection. But it stops being helpful when pain lingers, spreads, or flares up long after tissues should've calmed down. Many people with back pain, neck pain, sciatica, arthritis, or post-accident pain end up trapped between two frustrating messages: “Just rest it” or “Your scans don't look that bad.”
Neither one explains what you're feeling.
Pain neuroscience education offers a different path. It teaches you how pain works in the nervous system, why pain can stay active even when damage isn't getting worse, and how understanding that process can help you move with less fear and more confidence. This isn't about talking yourself out of pain. It's about learning how your body's protection system can become overprotective, then working to calm it down.
That matters because persistent pain is common. A review on pain neuroscience education notes that 25.3 million adults in the United States live with daily chronic pain, and it describes PNE as a vital non-pharmacological approach designed to teach the biological and physiological processes behind pain, rather than relying only on older models that equate pain with tissue damage (reviewed overview of PNE).
Rethinking Pain Beyond Tissue Damage
If you've ever said, “I don't get it. Why am I still hurting?” you're asking the right question.
The old model says pain is a direct readout of injury. Tissue gets irritated. Nerves send a signal. You feel pain. That does happen, especially early on. But with persistent pain, the system often becomes more complicated. The body may heal enough for normal activity, yet the pain alarm keeps sounding.
When the pain story stops making sense
In these situations, many people feel dismissed. They hurt when they bend, sit, walk, sleep, or lift, but imaging may not fully explain their symptoms. Or the findings sound scary without telling them what to do next. They start avoiding movement “just in case,” which can make the body stiffer, less confident, and more sensitive.
Pain neuroscience education changes the question from “Where is the damage?” to “Why is my system staying on alert?”
That shift can feel relieving. It doesn't deny pain. It gives pain a more complete explanation.
Pain can be real, intense, and disruptive even when it isn't acting as a precise measure of ongoing tissue harm.
A more useful model for persistent pain
PNE teaches that pain is a protective response shaped by the brain and nervous system. The body gathers information from tissues, stress, sleep, past experiences, beliefs, and environment. Then it decides how much protection to produce. Sometimes that response is well matched to the situation. Sometimes it's louder than necessary.
That's why two people can have similar scans and very different pain experiences. It's also why pain can flare during stress, poor sleep, or after doing an activity you've come to fear.
This approach provides control because systems can change. A sensitized alarm can become less sensitive. A fearful movement can become safe again. Recovery isn't only about “fixing a body part.” It's also about retraining the way your nervous system interprets and responds to threat.
Understanding Your Body's Pain Alarm System
A helpful way to think about pain is to compare it to an alarm.
A well-working alarm is protective. A smoke detector should go off when there's real smoke. A car alarm should react to an actual break-in. But if that same alarm starts blasting because of a leaf, a gust of wind, or a passing truck, the system isn't useless. It's too sensitive.
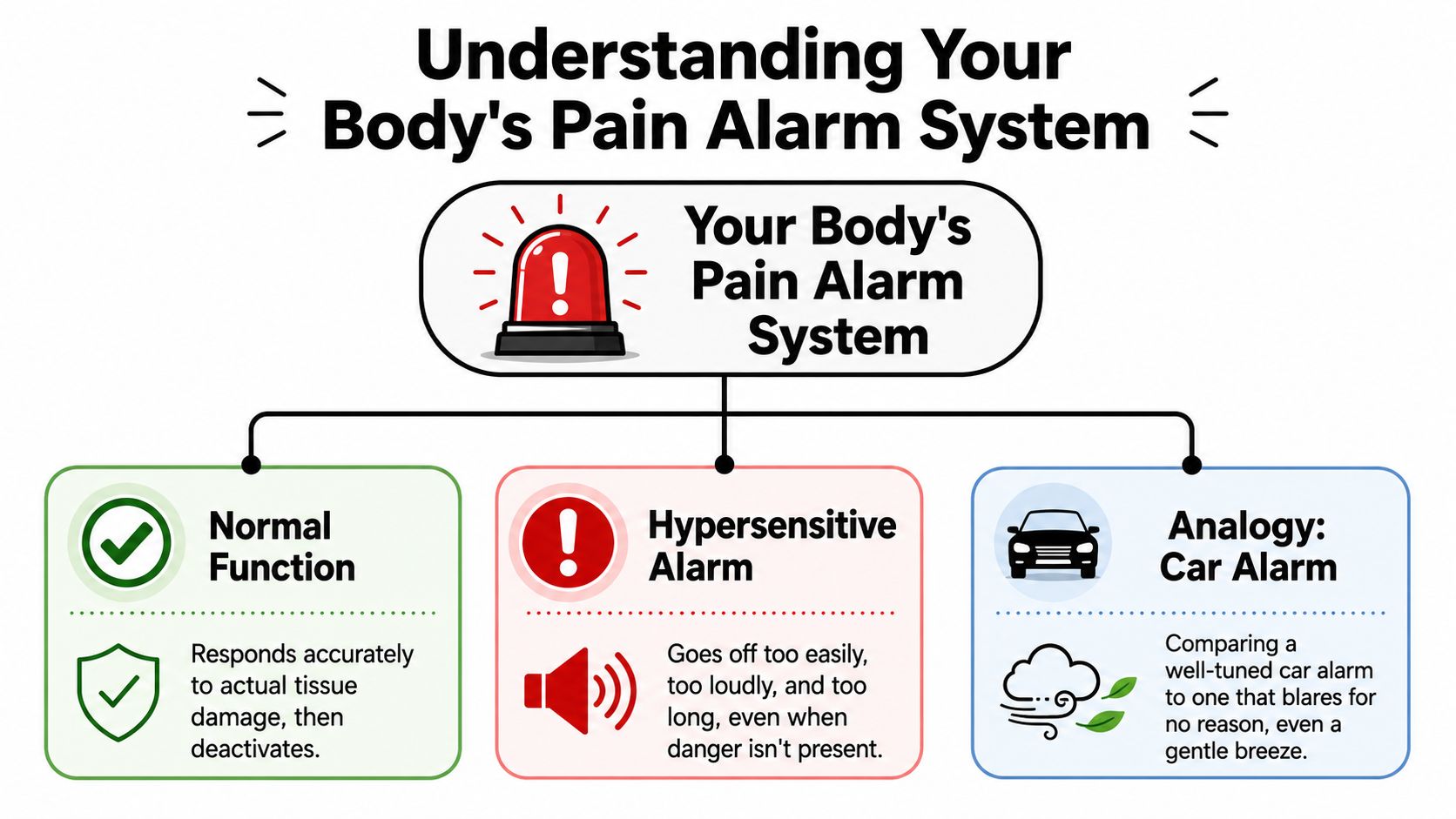
Normal alarm versus hypersensitive alarm
In an acute injury, pain often matches the moment. You twist your back, your body protects the area, and movement feels guarded for a while. That's useful.
In persistent pain, the nervous system can become more watchful. The threshold for danger drops. Activities that used to feel ordinary, getting out of a chair, turning your neck, carrying groceries, may start triggering pain more easily. The tissues may not be in fresh danger, but the alarm behaves as if they are.
This doesn't mean the pain is imagined. It means the protection system has become overactive.
A strong explanation of body awareness can help people notice this difference between sensation, threat, and movement habits. That's part of why clinicians often pair PNE concepts with body awareness training.
Pain is produced, not simply transmitted
Many people hear “the brain is involved” and think, “So you're saying it's all in my head.”
No. That's not what PNE means.
Your brain is part of every pain experience because it's the organ that interprets information and decides how much protection to create. That's a normal biological process. Pain is real, physical, and influenced by many inputs. If your system decides a movement is threatening, you may feel very real pain, muscle guarding, tension, and fatigue.
Practical rule: Hurt doesn't always equal harm, especially when pain has been around for a while.
A better question during rehab is often: “Is this movement dangerous, or is it unfamiliar and protected?”
That distinction helps people return to activity without ignoring symptoms or pushing recklessly.
A short visual explanation can make that idea click for many patients:
What confuses people most
Here are the sticking points I hear most often in clinic:
- “If movement hurts, shouldn't I stop?” Sometimes yes, briefly. But long-term avoidance can teach the nervous system that normal activity is dangerous.
- “If scans show wear and tear, doesn't that prove the pain?” Not always in a straightforward way. Structural findings and pain don't line up neatly for many people.
- “If stress changes pain, is it emotional?” Stress is physical. It changes tension, breathing, sleep, attention, and nervous system sensitivity.
Once people understand the alarm system, pain becomes less mysterious. And when pain feels less threatening, movement often becomes more possible.
The Proven Effectiveness of Pain Neuroscience Education
Understanding pain isn't just interesting. It can change outcomes.
When pain neuroscience education is combined with movement-based care, the research becomes much more compelling than education alone. That's an important point, because many people assume learning is separate from treatment. In reality, understanding pain can make treatment easier to tolerate and easier to stick with.
What the research shows
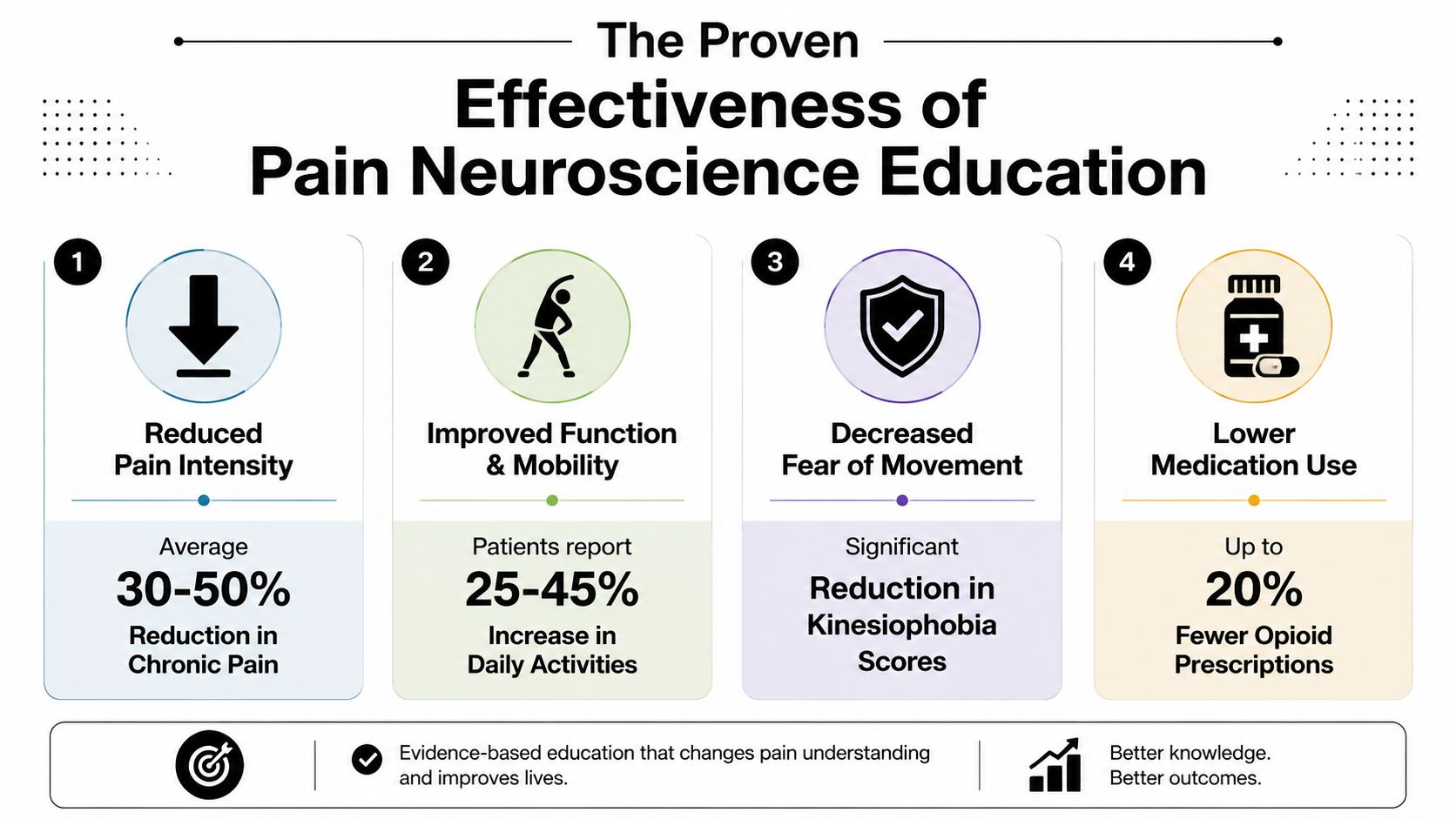
A review of 19 randomized controlled trials found that when pain neuroscience education was combined with therapeutic exercise, mean pain scores decreased from 5.89 before treatment to 3.03 after treatment, and mean disability scores improved from 56.67 to 12.51 (systematic review and meta-analysis on PNE with exercise).
Those numbers matter because they reflect two things patients care about most:
| Outcome | Before intervention | After intervention |
|---|---|---|
| Pain intensity | 5.89 | 3.03 |
| Disability score | 56.67 | 12.51 |
This same review also describes the pain reduction evidence as moderate certainty using GRADE evaluation. In plain language, that means the benefit isn't based on guesswork or a single promising paper. There's meaningful support behind it.
Why education changes pain
Pain neuroscience education helps reduce the “danger meaning” attached to symptoms.
If every ache feels like proof of worsening damage, the nervous system stays guarded. People brace, avoid, stop exercising, sleep poorly, and monitor every sensation. That cycle can keep pain going. When a therapist explains why your back can hurt without being fragile, or why a flare doesn't automatically mean re-injury, the threat level drops.
That lower threat response can help with:
- Fear of movement: A person becomes more willing to bend, reach, walk, or exercise.
- Catastrophic thinking: Sensations feel less alarming when they make sense.
- Activity tolerance: The body often moves more smoothly when it's not constantly bracing.
- Participation in rehab: People tend to engage better when treatment feels safe and logical.
Understanding pain doesn't erase symptoms overnight. It changes the context around the symptoms, and that can change what your nervous system does next.
Education works best as part of a plan
One of the biggest misconceptions about PNE is that a good explanation alone should fix chronic pain. For some people, that idea creates disappointment. For others, it leads them to keep searching for the perfect video, podcast, or worksheet.
A better frame is this: education helps open the door. Then movement, pacing, exposure, and hands-on care help you walk through it.
When the nervous system becomes less threatened, exercises feel less intimidating. Manual techniques may feel more tolerable. Daily activity becomes less of a fight. That's why PNE tends to work best when it supports a broader rehabilitation plan rather than replacing one.
What to Expect During Your PNE Sessions
Many individuals imagine education as a lecture. That's not what a good PNE session feels like.
It usually feels more like a conversation with someone who's trying to understand your pain story, how your symptoms behave, what you've been told before, and what movements or situations now feel risky to you. The therapist listens for patterns. Maybe your back pain spikes when you sit and stress is high. Maybe your neck pain flares more when you're tired. Maybe you move stiffly because you're afraid of “throwing it out” again.
A typical session feels collaborative
A therapist might sketch a simple diagram of the nervous system. They may use an analogy like a dimmer switch, a smoke detector, or an overprotective alarm. Then they connect that idea to your daily life.
For example, if lifting your laundry basket scares you, they won't just say “don't worry about it.” They might explain why the body braces when a movement feels threatening, how that guarding can increase symptoms, and how graded practice can rebuild safety.
You can learn more about the practical flow of a first rehab visit in this overview of what to expect during physical therapy.
Questions you might hear
Instead of focusing only on “where does it hurt,” a PNE-informed clinician may ask:
- “What do you think is happening when the pain starts?”
- “Which activities feel unsafe now?”
- “What have you stopped doing because of pain?”
- “What words have other providers used to describe your body?”
Those questions matter. The language people hear can shape the way they move. If someone believes their spine is unstable, their knee is worn out, or their neck is fragile, their nervous system may respond with more protection.
Who often benefits
PNE is often useful for people with persistent musculoskeletal pain, especially when the symptoms don't fully make sense through a simple tissue-damage model. That can include chronic low back pain, neck pain, arthritis-related pain, fibromyalgia, pain after an auto accident, or lingering symptoms after surgery or a healed injury.
It's also helpful for people who say things like:
| Common concern | What it may reflect |
|---|---|
| “I'm afraid to move the wrong way.” | A system that associates movement with danger |
| “Every flare makes me think I damaged something again.” | Threat-based interpretation of symptoms |
| “I've rested a lot, but I'm not improving.” | Protection that may now be too strong |
A good session should leave you feeling more informed, not blamed. You should feel that your pain has been taken seriously and explained in a way that gives you a path forward.
Practical Self-Management Tips to Retrain Your Pain System
Self-management doesn't mean you're on your own. It means you have tools to support what you're working on in treatment.
That distinction matters because pain neuroscience education is often marketed like a standalone fix, even though the data consistently shows education alone is much less effective than when it's paired with exercise or manual therapy. The PNE+ approach is the stronger one (clinical discussion of why PNE works best when integrated with care).
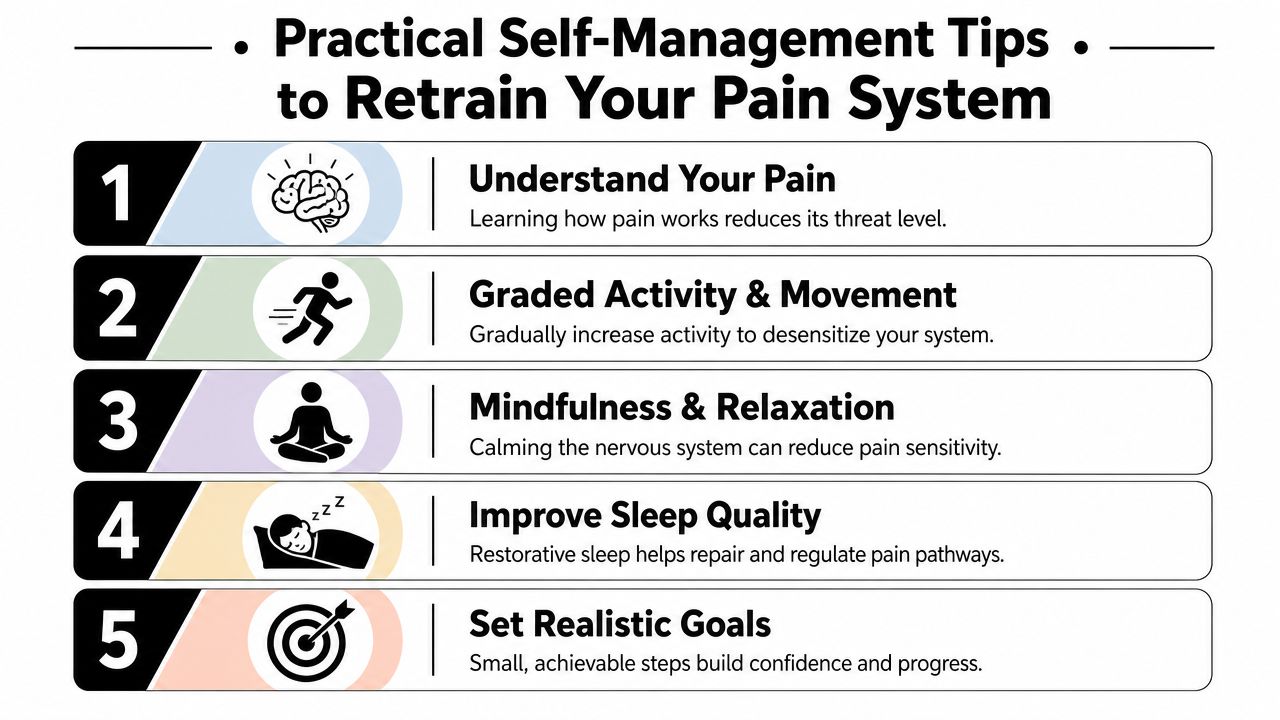
Five ways to turn down the alarm
Change the question you ask yourself.
Instead of “What did I damage?” try “What may have sensitized my system today?” Poor sleep, stress, overdoing activity, and fear can all raise the volume.Return to movement gradually.
If a task feels threatening, break it into a smaller version. Sit-to-stand from a higher chair. Walk for a shorter time. Reach halfway before reaching overhead. Success teaches safety.Use calm breathing during flare-ups.
Slow exhaling can reduce whole-body tension. That won't magically erase pain, but it may help your system stop escalating.Respect flare-ups without panicking.
A flare is often an increase in sensitivity, not automatic proof of new injury. Reduce load, keep some gentle motion, and resume progression once things settle.Track wins that aren't just pain scores.
Better walking tolerance, easier stairs, less fear, improved sleep, and faster recovery after activity all count.
Some of the best progress signs are quieter than pain relief at first. You may move more normally, recover faster, or feel less afraid before pain changes in a big way.
A simple flare-up response
When symptoms spike, people often bounce between two extremes. They either push hard and regret it, or stop everything and become more guarded. A middle path usually works better.
Try this sequence:
- Reduce the intensity, not all activity. Keep gentle movement in the day.
- Use reassuring language. “This is a flare, not automatically harm.”
- Return to your baseline plan. Resume the level of movement you were tolerating well.
- Build again in small steps.
What not to do
These habits often keep the alarm loud:
- Constant body checking: Repeatedly scanning for pain can increase threat attention.
- Boom-and-bust activity: Doing too much on a good day often triggers a rough next day.
- All-or-nothing thinking: If you can't do the full workout, do the scaled version.
The goal isn't to ignore pain. It's to respond in a way that teaches your nervous system that your body is capable, adaptable, and not as fragile as the pain may suggest.
How PNE Enhances Your Treatment at MedAmerica Rehab
The strongest version of pain neuroscience education isn't education by itself. It's education woven into hands-on care and movement.
Research supports that point clearly. A review on chronic musculoskeletal pain found that PNE shows a moderate-to-large effect size for reducing pain intensity when it's combined with exercise-based multimodal care, while PNE delivered in isolation doesn't show the same benefit. The paper describes this integrated model as PNE+, meaning education paired with treatments such as manual therapy, graded motor imagery, and neurodynamics (review of PNE+ for chronic musculoskeletal pain).

Why education makes hands-on care more useful
If your nervous system expects threat, even helpful treatment can feel intense, uncertain, or stressful. When you understand what's happening, your body often receives treatment differently.
Think about these common pairings:
| Treatment approach | How PNE can support it |
|---|---|
| Physical therapy | Helps you understand why graded exercise is safe and why soreness doesn't always mean setback |
| Chiropractic care | Reduces fear around movement and can make spinal or joint work feel less threatening |
| Acupuncture | Reframes unfamiliar sensations as therapeutic input rather than something alarming |
| Shockwave therapy | Gives context for treatment sensations so you can stay calmer and less guarded |
What this looks like in practice
A patient with low back pain may tense up during exercise because bending has become associated with danger. PNE helps reframe that movement. Once fear drops, the person can practice mobility and strengthening with better form and less guarding.
Someone recovering from an auto accident may interpret every flare as proof that something was “put back out.” Education helps explain why the nervous system can stay on high alert after trauma. That understanding can improve tolerance for manual therapy and structured exercise.
Another person may be hesitant about acupuncture or shockwave because the sensations are unfamiliar. When a clinician explains what the treatment is intended to do, and why temporary discomfort isn't automatically harmful, the experience often becomes less stressful.
Treatment tends to work better when your body experiences it as input for recovery, not as another threat to survive.
Why individualized plans matter
PNE shouldn't sound copy-and-paste. A retired golfer with arthritis, a warehouse worker with sciatica, and a patient recovering from shoulder surgery won't need the same explanation or the same exercise progression.
That's why integrated rehab works best when the education matches the person in front of you and the treatments fit your goals, irritability, and history. A helpful rehab plan doesn't just ask what hurts. It asks what you're trying to get back to, what your system currently tolerates, and what combination of education, movement, and manual techniques is most likely to help.
For patients looking for coordinated care rather than isolated treatments, it's worth understanding how clinics build individualized treatment plans around those factors.
Your Pain Neuroscience Education Questions Answered
Is pain neuroscience education only for chronic pain
It's most often used for persistent pain, but the ideas can help in earlier stages too. People recovering from an injury, surgery, or auto accident may benefit from understanding pain so they don't become overly fearful of normal rehab discomfort.
Does PNE mean my pain is psychological
No. PNE doesn't dismiss pain. It explains that pain is a real protective response shaped by the nervous system, not merely a direct tissue meter.
How quickly do people notice a difference
Some people feel relief as soon as the pain starts making more sense. For others, the bigger change comes later, when they begin moving with less fear and pairing the education with treatment. The timeline varies because pain sensitivity, habits, stress, sleep, and physical conditioning vary.
Can I just learn this online by myself
Online resources can help, but they can't tailor the message to your symptoms, beliefs, movement patterns, and treatment tolerance. A clinician can correct misunderstandings, adapt the explanation, and connect it to what you're doing in rehab.
Will I still need exercise or hands-on treatment
Usually, yes. PNE works best when it's integrated into a broader care plan rather than used as a standalone strategy.
What if I've been told my body is worn out
That message can make anyone afraid to move. But “wear and tear” language often creates more fear than clarity. A good clinician can put those findings into context and help you rebuild confidence in movement.
Is this approach appropriate for older adults
Often, yes. Older adults with arthritis, balance concerns, or fear of falling may benefit from understanding how pain and movement confidence interact. The explanation must match the person's goals and communication style.
If pain has been running your schedule, your sleep, or your confidence, you don't have to figure it out alone. MedAmerica Rehab Center helps patients connect pain neuroscience education with physical therapy, chiropractic care, acupuncture, and shockwave therapy in a practical treatment plan built around real daily function. If you're ready to understand your pain more clearly and start moving forward with support, reach out to schedule a consultation.