Fall Risk Assessment for Elderly: A Complete Guide
More than one in four adults age 65 and older fall each year. For many families, that number changes the conversation right away. Falls are common, but they are not something you have to accept.
A fall risk assessment for elderly adults helps turn worry into a plan. It looks at balance, strength, walking, medications, vision, and the home setup in the same way a home safety check looks at several small problems before they become one big one. The goal is not to label someone as frail. The goal is to spot what can be improved while confidence and independence are still strong.
Many seniors and family members worry that an assessment means bad news is coming. In practice, it is much more useful than that. It answers everyday questions in plain terms. Is it taking more effort to rise from a chair? Does turning too quickly cause unsteadiness? Could a medication or blood pressure change be adding dizziness? Is the bathroom arranged in a way that makes slips more likely?
Those answers give you something concrete to work with.
A good assessment does more than identify risk. It helps seniors and the people who care about them choose the next right steps, one by one, so daily life feels safer and more manageable, not smaller.
Why a Fall Risk Assessment is Your First Step to Safer Aging
After one fall or even one close call, the chance of another fall often rises. That is why waiting for a more serious incident can cost a family time, confidence, and options.

A fall risk assessment gives you a way to act early. It helps you respond to warning signs while they are still small and easier to address. In the clinic, I often compare this to hearing an unusual sound in a car. A quick check early on can prevent a much bigger problem later. Balance works in a similar way. Small changes in strength, vision, blood pressure, or reaction time can show up before a major fall happens.
Families often tell me they worry an assessment will label their loved one as frail. In practice, it works more like a map. It shows where the bumps in the road are, which routes feel safest, and what support will make daily movement feel steadier. That shift matters. You move from guessing to making decisions with a clear reason behind them.
It’s a starting point for practical action
A fall risk assessment is a structured look at how a person moves, what symptoms show up during the day, and which situations make balance harder. It is less like a school test and more like a careful tune-up.
That process can uncover patterns that are easy to miss at home, such as:
- Standing up and feeling lightheaded: a clue that blood pressure or timing may be part of the problem
- Losing balance during a quick turn: often a sign that coordination or leg control needs attention
- Walking well until doing two things at once: such as carrying laundry while answering a question
- Managing flat floors but struggling with curbs or stairs: a common sign that strength or confidence is changing
One practical rule helps many families. If someone has fallen, nearly fallen, or started avoiding normal activities because they feel unsteady, it is a good time to ask for help from a clinician trained in physical therapy for balance and mobility concerns.
The Goal: Building Confidence
A useful assessment does more than point out risk. It helps turn risk into a plan.
That difference is reassuring. If the main issue is weaker leg muscles, you can work on strength. If poor lighting is the problem, you can change the home setup. If dizziness started after a medication change, that gives you a clear question to bring to the prescribing clinician. Each answer leads to a next step that feels specific and manageable.
This is why fall prevention should be viewed as a confidence-building process for seniors and families. The aim is to help someone keep doing the things that matter, with better safety, better support, and less fear.
Understanding the Core Components of an Assessment
A good fall risk assessment for elderly adults is like a safety inspection for the body’s movement system. It looks at several parts together, because balance doesn’t depend on just one thing. Muscles matter. Vision matters. Blood pressure matters. Past falls matter. So does the home setup.
That’s why the process usually feels more like a conversation plus a set of movement checks than a single medical test.
Screening and full assessment aren’t the same
A quick screening asks, “Should we look closer?”
A full assessment asks, “What exactly is increasing this person’s risk, and what should we do about it?”
Here’s a simple comparison:
| Type | What it does | What it may include |
|---|---|---|
| Screening | Flags possible concern | A few questions about falls, dizziness, or walking difficulty |
| Comprehensive assessment | Builds a full picture | Health history, medication review, walking observation, balance and mobility testing, home safety discussion |
A primary care office, community event, or family conversation may start with screening. A therapy clinic often performs the deeper evaluation, especially when there’s already been a fall, repeated stumbles, or growing fear of movement.
The main pieces clinicians look at
A thorough assessment usually includes several layers.
- Fall history: The therapist asks whether there have been falls, near-falls, or moments of grabbing furniture to stay upright.
- Medical background: Conditions that affect strength, sensation, joints, blood pressure, or thinking can all influence safety.
- Medication review: Some medicines can contribute to dizziness, sleepiness, or slower reactions.
- Functional movement: The therapist watches how the person stands, walks, turns, and changes direction.
- Balance under real-life demands: Small challenges can show where steadiness breaks down.
For many people, this starts with familiar movements. Sitting down. Standing up. Taking a short walk. Turning around. Reaching. Looking up. None of that is meant to embarrass anyone. It helps the clinician see the gap between what the body needs to do and what it can safely do right now.
A useful assessment doesn’t reduce a person to a score. It connects symptoms, movement, habits, and environment into one clear picture.
Why collaboration matters
The best evaluations aren’t done to someone. They’re done with them.
A therapist may ask questions that seem simple, such as, “Do you feel less steady in the dark?” or “Do you avoid carrying things on the stairs?” Those details often reveal more than a formal test alone. They show how balance works in daily life, where confidence drops, and where treatment can make the biggest difference.
If you’re exploring options for mobility support, physical therapy services often include this kind of movement-focused evaluation and follow-up care.
Identifying the Most Common Fall Risk Factors
Falls rarely come from one cause. Most happen because several smaller problems stack up at the same time. A person may have mild leg weakness, slightly slower reactions, poor lighting in the hallway, and shoes that don’t fit well. Any one factor might seem minor. Together, they can create a real hazard.
One study of rural older adults found that being over 80 raised the odds of falling by 3.8 times, and postural hypotension raised the odds by 59.8 times, according to this analysis of fall risk factors in older adults. That doesn’t mean every older adult with these risks will fall. It means some factors deserve close attention because they can strongly shift the odds.

Body-related factors
Some risks come from changes inside the body.
Aging can affect muscle strength, reaction time, joint motion, and the ability to feel where the feet are on the ground. Vision can change too. If the eyes don’t pick up edges, shadows, or depth well, the brain gets less reliable information for balance.
A few common examples include:
- Lower body weakness: trouble rising from a chair, climbing stairs, or recovering after a trip
- Balance loss during turns: feeling steady walking straight but unsteady when changing direction
- Sensory loss in the feet: reduced feedback from the floor, which can make walking feel uncertain
- Blood pressure changes: dizziness or a “head rush” after standing up
For people living with diabetes, foot sensation and foot shape can play a major role in balance and walking safety. Family members who want a plain-language overview of diabetic foot complications may find that resource helpful for understanding why foot health affects stability.
Behavior and routine factors
Other risks come from how daily life is set up. These are often the most encouraging ones to discuss, because many can be changed.
A few examples stand out:
- Inactivity: less movement often leads to less strength and less confidence
- Unsafe footwear: loose backless shoes, worn soles, or shoes that slide on smooth floors
- Rushing: hurrying to answer the door, phone, or bathroom urge
- Ignoring mild dizziness: continuing to walk when the body is already signaling a problem
A person might say, “I’m careful, I don’t do anything risky.” But many falls happen during ordinary tasks. Getting dressed. Carrying groceries. Walking to the bathroom at night. Reaching into a cabinet. The routine nature of these moments is exactly why they can catch people off guard.
Fear can change movement too. When people become tense and overcautious, they may take shorter, less natural steps and move less efficiently.
Home and environment factors
The home can either support stability or work against it.
These are some of the hazards therapists often ask about:
| Area | Common problem | Why it matters |
|---|---|---|
| Stairs | Shoes, objects, or clutter left on steps | Increases tripping risk where recovery is hardest |
| Bathroom | No grab bars, slick surfaces | Reduces support during transfers and turning |
| Bedroom | Poor nighttime lighting | Makes orientation harder when getting up quickly |
| Living areas | Loose rugs or cords across walkways | Creates catch points for toes, canes, or walkers |
Environmental risks are important because they often don’t require major medical treatment. Sometimes the safest intervention starts with moving furniture, improving lighting, or changing footwear.
Why risk factors matter more in combination
Families often become confused. They may focus on one obvious problem and miss the pattern.
A person may say, “Dad’s balance is fine. He only fell because he got up too fast.” But getting up too fast may be connected to low blood pressure, weak legs, rushed movement, and a dark hallway. Looking at the whole picture is what makes a fall risk assessment for elderly adults so useful. It helps identify the combination, not just the incident.
What to Expect During a Comprehensive Evaluation
A common initial observation during a fall evaluation is that it feels calmer than expected. There’s no dramatic machine, no intimidating setup, and no trick. The therapist is watching how everyday movement works and where it starts to break down.
This visual gives a helpful overview of the process.
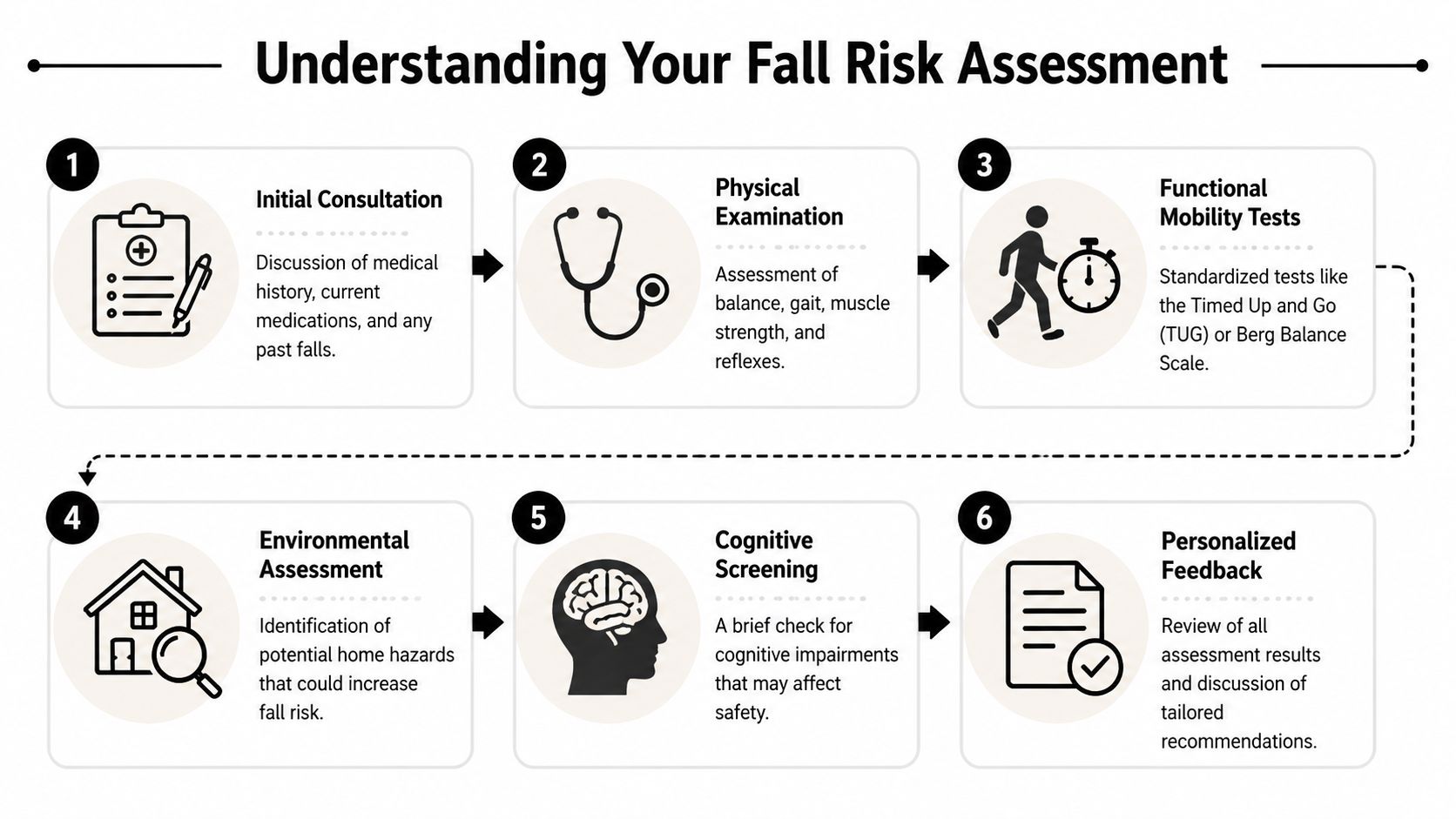
The appointment usually starts with conversation
A therapist often begins with questions that sound simple but matter a great deal.
They may ask:
- What happened during the last fall: Was there a trip, a faint feeling, a missed step, or a sudden turn?
- When unsteadiness shows up: At night, on stairs, after standing, outdoors, or in crowded places
- What has changed lately: New medications, new pain, new fear, or less activity
- What the person avoids now: Showers alone, walks outside, carrying laundry, or community outings
These details help separate occasional clumsiness from a true pattern. They also show whether the main issue is balance, strength, blood pressure, confidence, attention, or home setup.
Then come the movement tests
One common tool is the Timed Up and Go, often called the TUG. The person stands up from a chair, walks a short distance, turns, walks back, and sits down. To the patient, it feels like a normal task. To the therapist, it reveals several things at once. Leg strength, turning control, walking rhythm, and how steady the person is during transitions.
Another part of the visit may include standing balance tasks. The therapist might ask the person to stand with feet in different positions, reach gently, or shift weight. They may also observe normal walking speed and the way the feet clear the floor.
A structured tool may also be used to organize findings. The Hendrich II Fall Risk Model has demonstrated 78.72% sensitivity, according to the Hendrich II overview from Hartford Institute for Geriatric Nursing. In simple terms, that means it identifies many people who are at risk and gives clinicians a strong basis for planning intervention.
Some tests look easy from the outside. That’s the point. A small task can reveal a lot about how the body manages real-life movement.
A video can also help patients and families understand what screening and mobility checks may look like in practice.
What the therapist is actually looking for
Families sometimes think the therapist is just timing how fast someone moves. The deeper question is how safely and efficiently they move.
Here are examples of what clinicians notice:
| Observation | What it may suggest |
|---|---|
| Uses hands heavily to stand | Reduced leg strength or caution with balance |
| Takes many small steps to turn | Turning instability or fear of losing balance |
| Looks down constantly while walking | Reduced confidence, vision concerns, or habit compensation |
| Pauses before starting movement | Hesitation, dizziness, or uncertainty with weight shift |
These details are important because falls often happen during transitions, not during steady walking on a clear path. Standing up, turning, stepping backward, and navigating around furniture are common problem points.
Other parts of the evaluation
Depending on the setting, the therapist may also review footwear, ask about vision checks, or screen for how attention and memory affect safety. Some patients walk well when fully focused but become much less steady when talking, carrying something, or making a quick decision.
Occupational therapy can also be valuable when the concern extends into bathing, dressing, kitchen tasks, and home setup. If that’s part of the need, occupational therapy support can help address day-to-day safety in a very practical way.
What the visit should feel like
A strong evaluation should feel respectful. The clinician isn’t trying to prove frailty. They’re trying to understand function.
Most patients leave with a clearer sense of why they feel unsteady. That alone can be a relief. Uncertainty creates anxiety. Specific answers create options.
From Assessment Results to a Personalized Action Plan
Assessment only matters if it leads to action. The most useful outcome isn’t a label like “high risk.” It’s a plan that connects the findings to daily life and gives the person specific ways to move more safely.
A therapist takes all the pieces together. Fall history. Walking pattern. Balance test performance. Strength. Symptoms. Home barriers. Then they ask a practical question: what will lower risk and increase confidence for this specific person?
Turning test results into meaningful goals
One of the clearest examples is gait speed. A walking speed below 1.0 meter per second is a widely accepted benchmark for increased fall risk, according to this gait speed and fall risk summary. That matters because gait speed isn’t just a number. It reflects how efficiently the body organizes strength, balance, coordination, and confidence.
If gait speed is slow, the plan may focus on:
- Step quality: improving foot clearance and stride rhythm
- Posture in walking: reducing forward lean or guarding
- Turning practice: building control during changes in direction
- Endurance: helping the person maintain safe movement over longer distances
Someone else may walk at a reasonable pace but struggle every time they stand from a low chair. That points toward a different plan, often centered on lower body strength and repeated transfer practice.
A good plan should match the real problem
Personalized care is essential because the same fall could stem from very different causes.
Consider how different findings lead to different responses:
| Finding | Likely focus of treatment |
|---|---|
| Slow, cautious gait | Gait training, confidence-building walking practice |
| Poor stability while turning | Dynamic balance work and directional change practice |
| Difficulty getting up from chairs | Leg strengthening and transfer training |
| Unsafe home setup | Home changes, equipment choices, habit adjustments |
That last category matters more than many families expect. If the home keeps setting traps, exercise alone won’t solve the whole problem. For practical ideas, guides on aging in place home modifications can help families think through bathroom safety, lighting, handrails, and layout changes in a realistic way.
The best fall prevention plan doesn’t just make someone stronger in a clinic. It makes ordinary life easier and safer at home.
Confidence is part of the treatment
Fear changes movement. People who are worried about falling often stiffen up, shorten their steps, avoid activity, and gradually lose more strength. That creates a frustrating loop. Less movement leads to less capacity, which increases fear.
A thoughtful action plan breaks that loop gently. It might include supervised balance practice, safer ways to manage stairs, strategies for nighttime trips to the bathroom, or coaching on how to use a cane or walker more effectively. Progress is often built through repetition and small wins.
Examples of confidence-building targets include:
- Walking to the mailbox without rushing
- Getting out of bed and turning on lights before standing
- Standing from the dinner chair with better control
- Carrying light items while maintaining balance
These are not small things. They’re the building blocks of independence.
What families can do at home
Families don’t need to become therapists, but they can reinforce the plan well.
Helpful support often includes:
- Encouraging practice: reminding, not nagging
- Reducing clutter: especially around beds, bathrooms, and stairs
- Watching for patterns: dizziness, fatigue, or specific times of day when balance worsens
- Praising effort: noticing consistency, not just perfection
The action plan works best when everyone understands the goal. The goal isn’t to make life smaller. It’s to make movement safer, steadier, and less stressful.
Partnering with MedAmerica for Your Fall Prevention Journey
When balance changes start affecting daily life, local support matters. People do better when they can work with a team that listens closely, explains things clearly, and builds care around the person rather than around a generic protocol.
That’s one reason many families look for a clinic with hands-on therapy, individualized exercise, and experience treating older adults with mobility concerns. Fall prevention isn’t just about checking boxes. It’s about noticing how someone moves, what worries them, and what they want to keep doing in their daily life.
What good support should feel like
The right clinic experience should feel attentive, not rushed. A senior who’s worried about falling often needs more than instructions. They need reassurance, repetition, and practical guidance that makes sense in the context of their home and routine.
A helpful care team should be able to address questions like:
- Why do I feel unsteady when I turn?
- Why is getting up from the couch harder now?
- Should I be using a cane differently?
- What can I practice safely between visits?
That kind of clarity builds trust. It also makes it easier for patients to stick with treatment long enough to benefit from it.
Why a local senior-focused option matters
For older adults in Deerfield Beach, convenience and familiarity can make follow-through much easier. Travel stress, long waits, and unclear expectations often discourage people from getting started. A clinic that understands senior mobility concerns can remove many of those barriers.
If you’re looking for care built around balance training, walking support, and fall prevention, senior physical therapy in Deerfield Beach offers a more focused next step than waiting to see if the problem gets worse.
Good fall prevention care protects more than safety. It protects routines, confidence, and the ability to stay engaged in everyday life.
The most important thing is to act while the signs are still manageable. A near-fall, a growing hesitation on stairs, or a habit of holding furniture while walking all deserve attention. Early care often gives people more options and better momentum.
Your Questions on Fall Risk Answered
Families usually have the same few worries. They want to know when to act, what an assessment means, and whether asking for help will lead to loss of independence. In practice, the opposite is usually true. Clear answers give people more control, not less.
Frequently asked questions
| Question | Answer |
|---|---|
| When should someone get a fall risk assessment? | A good time is when there has been a fall, a near-fall, new dizziness, slower walking, more furniture-holding, or growing fear about stairs or bathing. You don’t need to wait for a serious injury to ask for help. |
| Does needing an assessment mean someone is frail? | No. It means there are signs worth checking. Many active older adults benefit from assessment because small changes in balance or walking can be hard to notice until they start affecting daily life. |
| Will the evaluation be painful or exhausting? | Most assessments involve conversation, simple standing and walking tasks, and observation of normal movement. The clinician should adjust the visit to the person’s ability and comfort. |
| What if my parent says they’re fine but keeps grabbing walls or furniture? | That behavior often tells you more than words do. Many people minimize symptoms because they don’t want to worry family members or admit they feel less steady. A calm, supportive conversation usually works better than arguing. |
| Can home changes really make a difference? | Yes. Better lighting, safer bathroom setup, clutter removal, and more supportive footwear can reduce unnecessary hazards and make daily movement easier. |
| Is a cane or walker a sign of giving up? | Not at all. The right device, used correctly, can increase safety and confidence. The key is proper fit and training, not just buying one and hoping for the best. |
| Can exercise still help if someone has already fallen? | In many cases, yes. Strength, gait training, transfer practice, and balance work can all be tailored after a fall, especially when guided by a professional evaluation. |
| What should family members watch for between visits? | Notice changes in speed, hesitation during turns, needing to push hard with the arms to stand, avoiding usual activities, or seeming unsteady in dim light or on uneven surfaces. |
A few concerns deserve a direct answer
Some people worry that documenting fall risk will automatically lead to restrictions. That isn’t the purpose. The purpose is to reduce preventable danger while keeping the person as active and independent as possible.
Others worry that the answer will only be “exercise more.” A good plan is much more specific than that. It should reflect how the person moves, what situations trigger unsteadiness, and what changes will fit realistically into daily life.
Asking for a fall assessment doesn’t take independence away. It gives you better information for protecting it.
If you’re unsure whether it’s time
Use common sense and trust patterns, not promises. If someone says, “I’m okay,” but they’ve started moving much more slowly, avoiding outings, or reaching for walls, those are meaningful clues. If a spouse says, “He seems different on the stairs,” that matters too.
The earlier you address balance concerns, the easier it usually is to build a plan around them. Waiting often makes the problem feel bigger and the person feel more nervous.
If you’ve been wondering whether to bring it up, that’s often your answer. It’s worth asking.
If you or someone you love has had a fall, a near-fall, or growing difficulty with balance, MedAmerica Rehab Center can help you take the next step with clarity and confidence. Their team provides personalized care focused on safer movement, stronger walking, and practical fall prevention strategies so seniors in Deerfield Beach can stay active and independent.