
Fall Prevention Exercises to Boost Balance
That uneasy moment often happens fast. You reach into a cabinet, step off a curb, turn too quickly in the kitchen, and your body has to scramble to catch up. Even if you don't fall, the experience can stay with you.
For many people, the bigger problem starts after the close call. You walk less, avoid stairs, hold back on errands, and start planning your day around what feels safest. That makes sense emotionally, but physically it can shrink your strength, your balance, and your confidence at the same time.
Fall prevention exercises help reverse that pattern. Done the right way, they train the exact systems that keep you upright: leg strength, balance reactions, walking control, and the ability to move with less hesitation. Falls are common. The American Public Health Association notes that Johns Hopkins Medicine reports more than 25% of adults age 65 and older fall each year, and about 3 million are treated in emergency departments for fall injuries annually in its falls prevention policy brief.
What generic guides often miss is this: many people who need balance work aren't starting from a clean slate. They have knee arthritis, back pain, neuropathy, a recent joint replacement, or lingering weakness after an injury. In those cases, the right starting point isn't the hardest exercise. It's the safest one you can perform well and repeat consistently.
Regaining Your Footing and Your Confidence
Losing confidence in your balance can change daily life more than people expect. You stop carrying laundry up the stairs. You pause before showering. You hold onto furniture when no one is watching. The body gets less practice moving, and everyday tasks start to feel less automatic.
That cycle is exactly why structured fall prevention exercises matter. They don't just “work on balance.” They rebuild the skills behind safe movement, such as standing up from a chair, shifting weight, walking in a straight line, and catching yourself when your body wobbles.
Fear changes movement
When someone feels unsteady, they usually move more stiffly. Steps get shorter. Turns get slower. The eyes drop to the floor. Those are understandable reactions, but they don't always improve control. In the clinic, we often see people brace so much that they stop using the normal ankle, hip, and trunk adjustments that help them stay upright.
Fear of falling can limit life before an actual fall does.
That's why a good exercise plan has two jobs. It needs to improve physical capacity, and it needs to restore trust in movement. If either piece is missing, progress tends to stall.
Progress starts smaller than most people think
A lot of people assume balance training means standing on one foot with no support or trying advanced drills too soon. That's not how safe progress works, especially if pain or post-surgical stiffness is part of the picture. The first wins are often simpler:
- Standing more evenly with both feet planted
- Rising from a chair without rushing
- Shifting weight calmly from side to side
- Walking with a steadier rhythm instead of guarding every step
Those basics don't look flashy. They work.
A Quick Self-Assessment for Your Starting Point
Before starting fall prevention exercises, it helps to get a realistic picture of where your balance is today. This isn't about diagnosing yourself. It's about choosing a starting level that's safe enough to practice and challenging enough to help.
Use a sturdy chair, wear supportive shoes, and stand near a counter or wall. If you've had recent falls, significant dizziness, or you feel unsafe doing these checks alone, skip the home testing and ask for professional guidance instead. If you want a more formal screening process, MedAmerica also explains what clinicians look for during a fall risk assessment for elderly adults.

Check one balance position at a time
Try these positions in order. Keep one hand close to support.
Feet apart
Stand with your feet about hip-width apart for a short hold. Notice whether you sway, grip the floor with your toes, or feel like you need support right away.Feet closer together
Bring your feet closer until they're almost touching. This narrows your base of support and asks your balance system to do more.Tandem stance
Place one foot in front of the other, as if standing on a line. If that's too hard, widen the distance between the feet slightly.Single-leg stand
Lift one foot just off the ground while keeping a hand near support. Don't force this if it causes pain or you feel unsafe.
What matters most isn't the number of seconds. It's the quality. If you're holding your breath, leaning hard on the counter, or feeling panicky, that's not your true training level yet.
Try a simple chair-and-walk check
Use a sturdy chair that doesn't slide.
- Sit tall with both feet on the floor.
- Stand up with control.
- Walk forward a short distance in a clear area.
- Turn slowly and return to the chair.
- Sit back down without dropping heavily.
Notice what feels difficult:
| What you notice | What it often suggests |
|---|---|
| You need to push hard with your arms | Leg strength may need attention |
| You feel unsteady on the turn | Dynamic balance and gait control may need practice |
| You sit down abruptly | Eccentric leg control may be limited |
| Pain shows up right away | You may need modifications before progression |
Use your result to choose a level
A useful way to sort your starting point is simple:
- Begin at level 1 if you need both hands near support, have active pain, or feel unsteady in narrow standing positions.
- Begin at level 2 if you can stand and walk independently but feel cautious with turns, uneven ground, or longer periods on your feet.
- Seek supervised care first if dizziness, numbness, post-surgical restrictions, or sharp pain are part of the picture.
Practical rule: Start where you can succeed with good form. Balance improves faster when your nervous system feels challenged, not threatened.
The Four Pillars of Fall Prevention Exercises
Fall prevention work goes better when it trains the body for real tasks. A strong program combines strength, balance, walking control, and mobility, rather than practicing one skill in isolation. A British Journal of Sports Medicine review supports that multicomponent approach, and it matches what we see in the clinic at MedAmerica Rehab Center, especially with patients who are dealing with arthritis, back pain, or recovery after surgery.
That last group often gets overlooked.
If standing exercises flare your knee, or if your hip still feels stiff after surgery, the answer is not to skip balance training. The answer is to start with the right version, at the right dose, with support close by.
Here's the big picture.

Strength keeps everyday movements controlled
Strength gives you the ability to stand up, lower into a chair, climb a step, and catch yourself when your body shifts unexpectedly. For many adults with pain or stiffness, this is the first place to build.
A practical starting exercise is the sit-to-stand.
How to do it
- Sit on a sturdy chair.
- Place your feet flat, slightly behind your knees.
- Lean forward from your hips.
- Press through your feet and stand up.
- Pause briefly.
- Lower yourself back down slowly.
A commonly used home exercise handout from Kaiser Permanente includes examples of repetition ranges, hold times, and walking drills often used in fall-prevention programs. The exact numbers matter less than the quality of the movement. Stand up without rocking hard or dropping back into the chair.
For knee arthritis, raise the seat with a firm cushion so you do not have to bend as much. After surgery, use the armrests lightly if needed and keep the motion in a comfortable range at first. Good form with a shorter range beats painful reps every time.
Balance teaches your body to recover
Balance training helps you stay centered over your feet when you reach, turn, or pause. It also helps your nervous system trust that you can handle small shifts without grabbing or freezing.
Start with supported narrow stance.
How to do it
- Stand at a kitchen counter or sturdy surface.
- Begin with your feet hip-width apart.
- Narrow your stance a little if that feels safe.
- Hold the position while breathing normally.
- Use your fingertips only if needed.
If that goes well, progress to a split stance or a light single-leg weight shift. Full single-leg standing is useful for some people, but it is not the first step for a painful knee, an arthritic hip, or a patient who is still guarding after surgery.
That trade-off matters. A harder balance drill is not better if it makes you brace, hold your breath, or grip the counter the whole time.
For readers who want a basic primer on how joints and muscles contribute to stable movement, this guide on explore healthy muscles and bones gives helpful context.
A short demonstration can also help make the movement patterns easier to picture.
Gait drills improve safety while you move
Many falls happen during walking, turning, or changing direction. That is why gait practice deserves its own pillar.
One useful drill is heel-to-toe walking, but it needs to match your current ability.
- Stand tall next to a counter or wall.
- Place one foot in front of the other with a small gap, or heel-to-toe if you can do it safely.
- Walk forward slowly.
- Keep your eyes forward.
- Reset and repeat.
If you feel unsteady, widen the distance between your feet. If you have foot pain, neuropathy, or limited motion after surgery, start with slower, deliberate walking in a clear hallway instead of a tight line. The goal is controlled steps, not forcing a challenge your body cannot organize yet.
I often tell patients this: walking drills should make you more fluid, not more tense.
Flexibility gives the other three pillars room to work
Mobility helps you use your strength and balance more efficiently. Stiff ankles, hips, or trunk rotation can make simple walking feel awkward and can limit your ability to recover from a small trip.
A safe place to begin is seated ankle mobility.
Try this:
- Sit in a chair.
- Lift one foot slightly.
- Make slow ankle circles in each direction.
- Keep the motion smooth.
- Repeat on the other side.
This exercise looks simple because it is simple. It is also useful. If your ankle does not bend well, your body often compensates by turning the foot out, shortening the step, or shifting stress up to the knee and hip.
For painful joints, stay in a gentle range and avoid pushing into a pinch or sharp pain. For post-surgical patients, follow the restrictions you were given. Mobility work should reduce barriers to movement, not irritate healing tissue.
Your Weekly Fall Prevention Exercise Routine
A good routine should leave you feeling practiced, not beaten up.
That matters even more if you are starting with knee arthritis, back pain, or a recent surgery. In the clinic, I usually start these patients with smaller doses than they expect. That is not being overly cautious. It is how you build consistency without causing a pain flare that makes you skip the next three days.
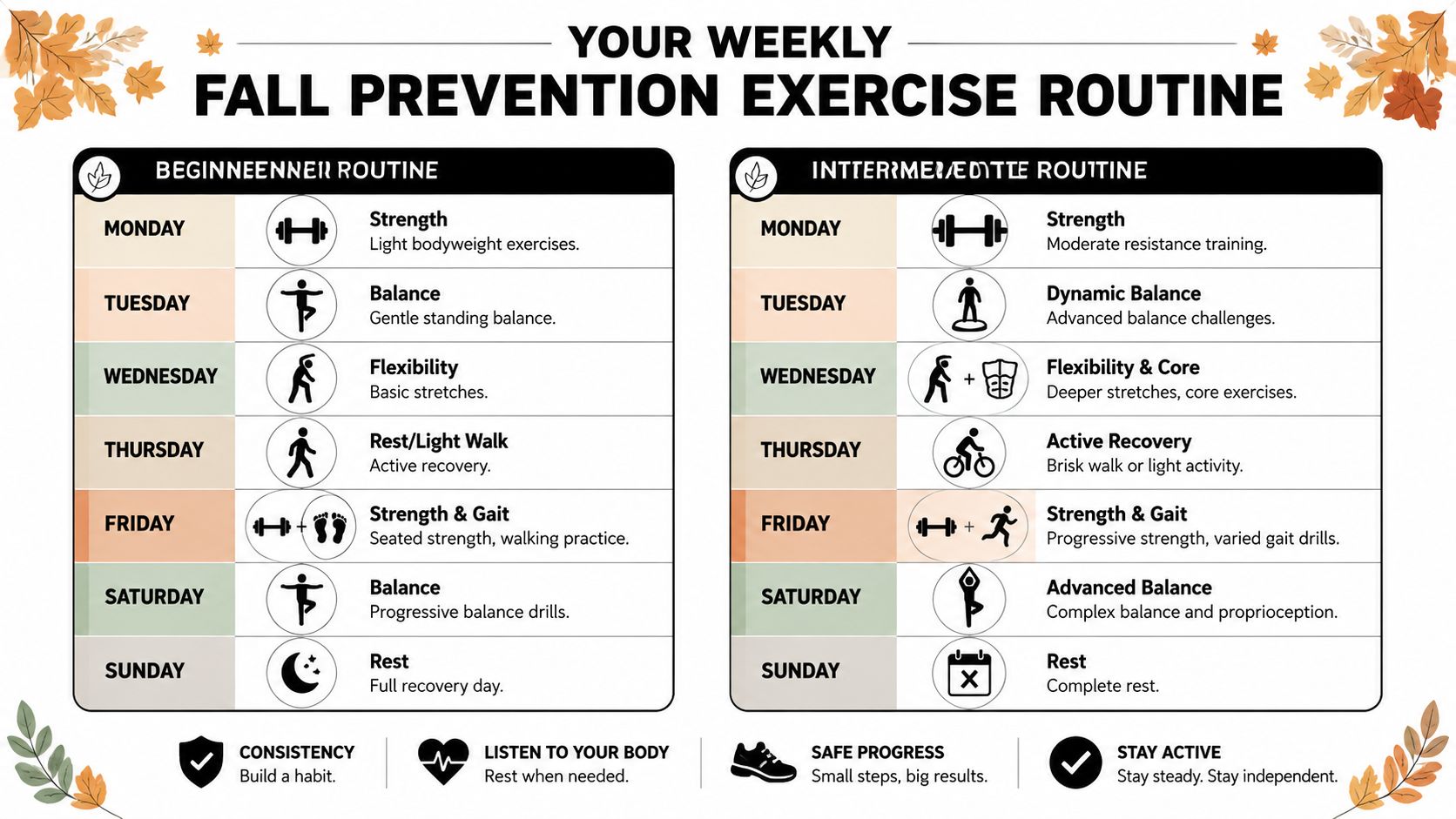
A beginner week that feels doable
If you are dealing with pain, stiffness, fatigue, or reduced walking tolerance, start with a week that gives you repeat practice and enough recovery.
| Day | Focus | Example |
|---|---|---|
| Monday | Strength | Sit-to-stands and gentle calf raises |
| Tuesday | Balance | Supported narrow stance and weight shifts |
| Wednesday | Mobility | Ankle circles and gentle walking |
| Thursday | Recovery | Light walk in a safe area |
| Friday | Strength and gait | Sit-to-stands plus heel-to-toe practice by a counter |
| Saturday | Balance | Repeat Tuesday with slightly less hand support if safe |
| Sunday | Rest | Full rest or easy movement around the house |
This schedule works well for painful or stiff joints because the harder days are separated. Your legs get time to settle down, and your balance system still gets frequent practice.
Keep the first two weeks boring on purpose. Familiar drills usually produce better form, better follow-through, and more confidence than constantly changing the program.
An intermediate week adds challenge with control
Progression should be specific. If your pain stays stable during exercise and later that day, and you can keep good form without grabbing suddenly for support, add one small change at a time.
Use these progressions:
- Lighten hand support from a full hand hold to two fingers.
- Narrow the base of support by bringing the feet a little closer together.
- Increase time or reps by adding a few more seconds or one more round.
- Use less arm help during sit-to-stands if your knees and hips tolerate it.
- Lengthen walking drills with a few extra passes in a clear hallway or along a counter.
Avoid stacking all of those changes into the same session. That is where people with arthritis, neuropathy, or post-operative weakness get into trouble. One variable at a time lets you tell whether your body handled the added challenge well.
A simple target works better than chasing hard workouts. For example, hold a balance position a little longer this week, or complete your sit-to-stands with smoother control. Progress is not about making the exercise look impressive. It is about making daily movement safer and easier.
If you finish your routine feeling steadier and only mildly tired, that is a good training dose. If your pain spikes, your form falls apart, or you feel less secure by the last round, reduce the challenge next time.
Add walking or cardio without derailing recovery
Walking is useful, but it is not the only option. If outdoor walking is limited by heat, rain, small living space, or joint pain, short indoor cardio sessions can help you keep moving between strength and balance days. For ideas you can adapt at home, this guide to high-ROI cardio exercises for gyms has several simple options.
Keep the dose modest. Ten calm minutes done regularly is better than one long session that leaves your knee swollen or your back irritated.
If home setup is part of the challenge, review these fall prevention tips for safer movement at home and pair them with your exercise plan. The routine works best when the exercises and the home environment support each other.
Safety First Modifications for Real Life
The most important part of fall prevention exercises isn't the exercise list. It's the setup. If the environment is unsafe, even a good drill becomes a bad choice.
That's why clinical guidance treats safety setup as part of the intervention itself. Exercises should be performed near a stable support like a countertop or wall so you have one-contact recovery available, as noted in this review on exercise interventions and safety setup.
Non-negotiable safety rules
Use these every time:
- Clear the area so rugs, cords, pet bowls, and clutter aren't in your path.
- Choose stable support like a heavy counter, sturdy chair braced against a wall, or solid railing.
- Wear proper footwear unless a clinician has told you to practice barefoot for a specific reason.
- Stop for sharp pain because balance work should challenge you, not provoke a pain spike.
- Practice when alert rather than when you're rushed, tired, or just took medication that makes you groggy.
If you use an assistive device, keep it within reach. If transfers are difficult, home equipment and support accessories may become part of the safety plan. In more advanced mobility situations, caregivers may need education on transfer equipment, and resources like this overview of Hoyer sling materials can help them understand support options.
How to modify common exercises
Pain or mobility limits don't mean you should skip training. They mean the exercise has to fit the body you have today.
With knee arthritis or knee pain
- Use a higher chair for sit-to-stands.
- Keep the movement slow and shallow at first.
- Focus on even weight through both legs.
- Avoid dropping into the chair.
With back pain or sciatica
- Keep your trunk slightly forward but not collapsed during standing tasks.
- Start with small weight shifts instead of long reaches.
- Shorten walking drills if symptoms spread down the leg.
After surgery
- Follow the surgeon's movement precautions first.
- Start with supported standing and controlled transfers.
- Don't add narrow stance or single-leg work until basic standing feels steady.
With neuropathy or reduced foot sensation
- Use more visual feedback by looking ahead at a fixed target.
- Practice near strong support.
- Prioritize slower transitions over longer holds.
A lot of people make the same mistake here. They think the goal is to “push through” because balance work is supposed to feel hard. It's supposed to feel challenging. It's not supposed to feel reckless.
For more home setup ideas beyond exercise technique, this guide on how to prevent falls at home covers practical environmental changes that support safer daily movement.
When to See a Physical Therapist in Deerfield Beach
You start a balance drill at the kitchen counter, then your knee flares, your back tightens, or you feel unsure shifting weight onto the leg that still does not feel normal after surgery. That is usually the point where a generic routine stops being helpful.
Home exercise works well for many people. It works best when the starting point matches your pain level, strength, sensation, and movement restrictions. If you have had a recent fall, ongoing dizziness, joint pain, neuropathy, or a recovery that feels slower than expected, an in-person assessment gives you a safer way to begin and a clearer way to progress.
Signs you shouldn't rely on a generic routine
Consider professional help if any of these apply:
- You've had a recent fall or near-fall and don't know why it happened
- You feel dizzy when turning, standing, or walking
- Pain increases during balance work instead of settling afterward
- One leg feels much weaker than the other
- You've had joint replacement or another surgery and aren't sure how to progress
- You stop exercising because it feels unsafe, confusing, or too painful
What a therapist adds
In the clinic, the first job is figuring out what is driving the balance problem. Sometimes it is leg weakness. Sometimes it is limited ankle motion, poor foot sensation, vestibular dizziness, pain guarding, or the habit of rushing transfers because movement feels hard. Those problems do not respond to the same exercise in the same dose.
That matters even more with arthritis, back pain, or post-surgical stiffness. A good program may start with easier sit-to-stands, shorter standing intervals, or gait work that builds confidence before it challenges balance. Slower progress can still be the right progress if it keeps symptoms settled and lets you practice consistently.
A physical therapist can:
- Set the right starting level based on what you can do safely today
- Work around pain and precautions after surgery or with chronic joint and spine issues
- Correct movement mechanics during transfers, walking, turning, and reaching
- Progress difficulty safely as strength, control, and confidence improve
MedAmerica Rehab Center provides physical therapy for balance and gait problems, post-surgical rehabilitation, and fall-prevention training in Deerfield Beach. If you are comparing options, this guide on how to choose a physical therapist gives you practical questions to ask before you book.
The right plan should help daily movement feel steadier and less stressful.
If you are avoiding walks, holding onto furniture, or cutting back activity because pain and balance problems feed into each other, a physical therapist can help you sort out what to modify, what to strengthen, and what to leave alone for now. That kind of guidance often makes the difference between exercising once in a while and building a routine you can stick with.