
Trigger Point Therapy: Lasting Pain Relief
You wake up with a stiff neck, roll your shoulder, and feel a sharp spot that seems too small to cause this much trouble. By noon, that same area is feeding a headache, making your desk setup feel unbearable, and turning simple movements into a constant reminder that something isn't right.
That pattern is common in clinic. A lot of people don't have a major injury. They have a muscle that never fully let go. The pain feels mysterious because the sore spot and the place you feel pain aren't always the same. That's where trigger point therapy can make sense, especially when it's used thoughtfully instead of as a one-size-fits-all fix.
What Are Trigger Points and Why Do They Hurt
A trigger point is a hyperirritable spot inside a taut band of skeletal muscle. The simplest way to picture it is a tiny knot in a rope. If one short section of the rope tightens and won't release, tension spreads through the whole line. Muscle behaves in a similar way. One small area stays contracted, the surrounding tissue gets stressed, and movement starts to feel restricted and painful.
Researchers describe myofascial trigger points as a foundational mechanism in musculoskeletal pain syndromes, and they're often activated by muscle overload, poor posture, or trauma, as described in this clinical review of myofascial trigger points. That fits what people experience in real life. Long hours at a laptop, a sudden increase in training, lifting with poor mechanics, or even guarding after an accident can all create the conditions for a trigger point to form.
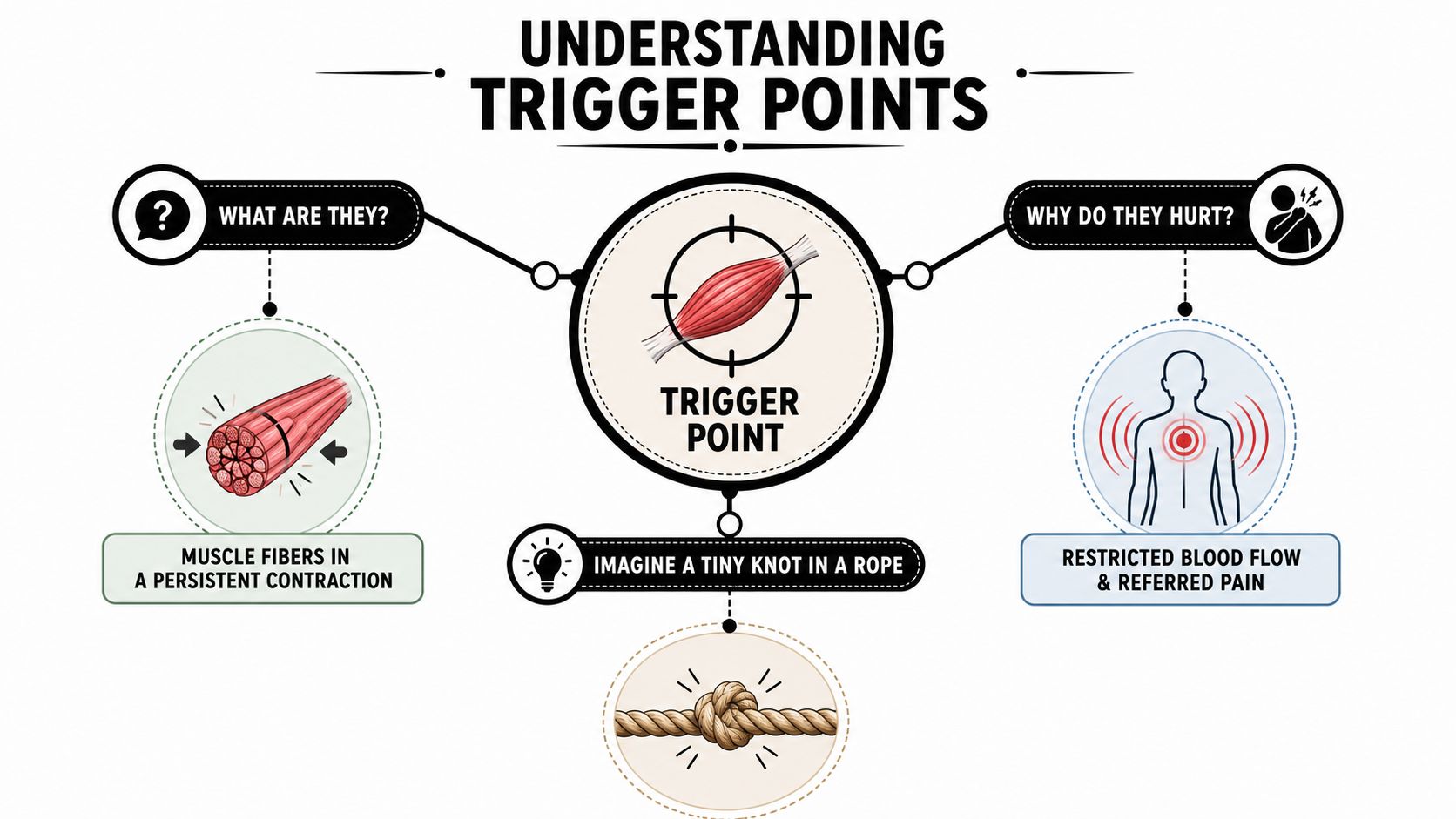
The pain isn't always where the problem lives
One reason trigger points are confusing is referred pain. Press on a spot in the upper shoulder, and the ache may travel into the neck or head. Work on a glute trigger point, and a patient may recognize the pull down the back of the leg that they thought was coming only from the low back.
That referral pattern matters because people often chase symptoms instead of the source. They stretch the painful area over and over, but the muscle that's driving the pain stays locked down.
A trigger point can be small, but the pain pattern it creates can feel much bigger than the spot itself.
Active and latent trigger points
Not every trigger point behaves the same way.
- Active trigger points cause ongoing pain, often enough to interrupt sleep, work, exercise, or concentration.
- Latent trigger points don't always hurt at rest, but they're tender when pressed and can limit motion, strength, or movement quality.
This is why someone can say, “I'm not in severe pain all day, but my shoulder just doesn't move right.” The muscle may still be guarding even when symptoms are quieter.
Why they keep coming back
A trigger point rarely appears for no reason. Common drivers include:
- Postural strain from sitting with the head forward or shoulders rounded
- Overload from sports, yard work, or a sudden jump in exercise intensity
- Protective tension after trauma, surgery, or joint irritation
- Repetitive use from work tasks, childcare, driving, or lifting
Sometimes trigger point therapy works best when paired with broader soft tissue work. If you want a clear overview of how that bigger tissue approach fits in, this guide on myofascial release therapy is a useful companion.
Exploring Professional Trigger Point Therapy Techniques
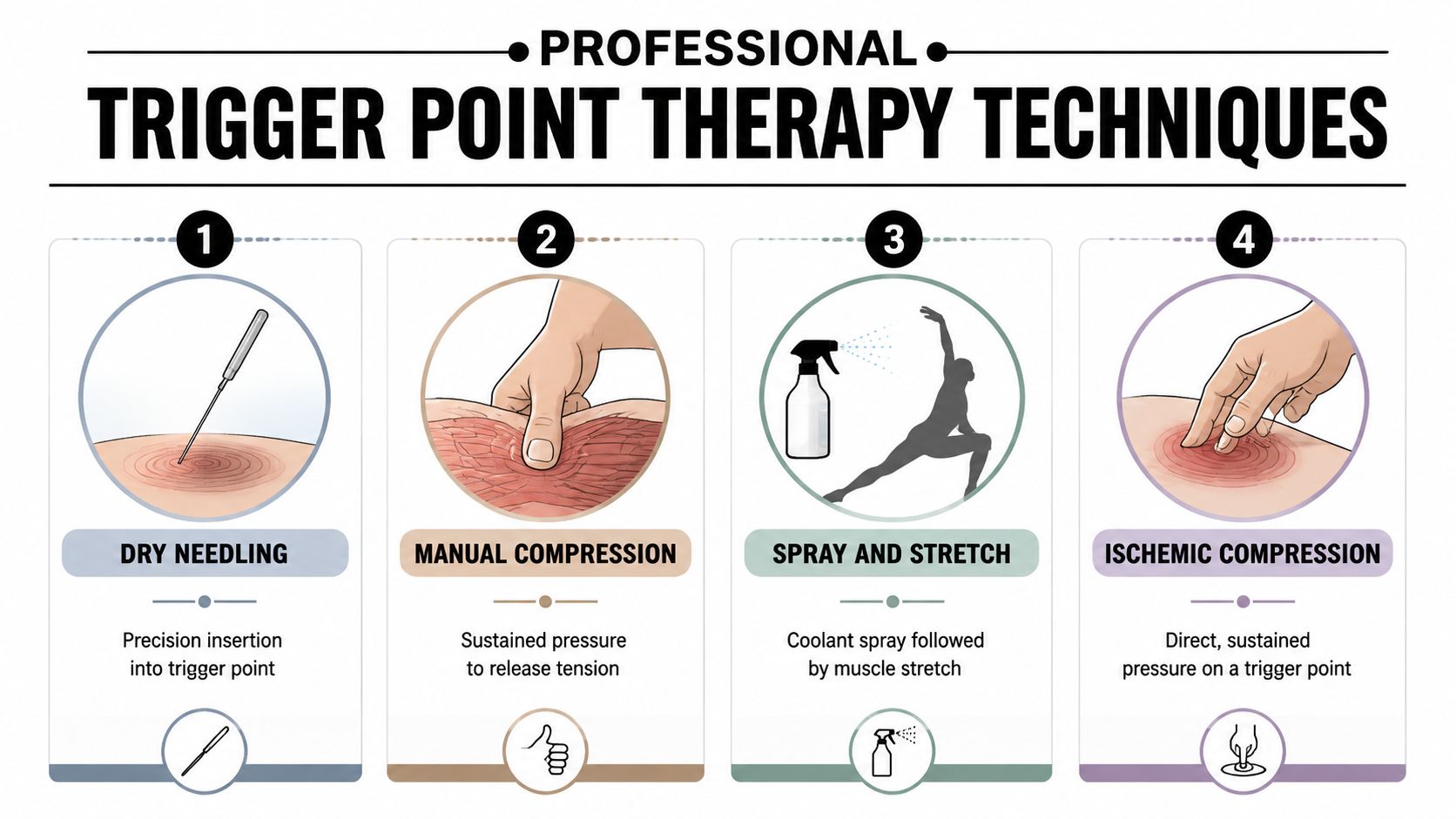
Patients often ask the same practical question. “What's the difference between hands-on release, dry needling, and injections?” The short answer is that they all target irritated muscle, but they do it in different ways and with different trade-offs.
Systematic reviews have shown that trigger point dry needling is often more effective than stretching or manual therapy alone for myofascial pain, while manual therapy has a moderate level of evidence for short-term relief, according to this summary of trigger point treatment evidence. That doesn't mean manual work is weak. It means technique selection should match the patient in front of you.
A side-by-side look at common options
| Technique | What it is | What it feels like | Best fit |
|---|---|---|---|
| Manual compression | Sustained pressure from a therapist's thumb, fingers, knuckle, or elbow | Deep, focused pressure that should ease as the tissue softens | Sensitive patients, first-line care, broad muscle tension |
| Dry needling | A thin needle targets the trigger point directly | Quick pinch, ache, or twitch sensation, followed by soreness or relief | Stubborn points that don't fully respond to hands-on work |
| Trigger point injections | A medical provider places medication into the painful point | Brief needle discomfort, then localized soreness | Persistent cases that have plateaued with conservative care |
| Spray and stretch | A cooling spray followed by guided lengthening | Surface cooling with a stretch sensation | Muscles that are guarding and hard to lengthen comfortably |
Manual release and ischemic compression
This is the foundation of trigger point therapy in many physical therapy settings. The therapist finds the taut band, presses into the point, and holds pressure while monitoring your response. Good treatment feels targeted, not chaotic. The point is to persuade the muscle to release, not overpower it.
Manual release works well when the tissue is irritable, the nervous system is wound up, or the patient is nervous about needles. It also gives the therapist constant feedback. If the pain spreads, dulls, or softens under the hand, that tells us something useful.
Dry needling and when it earns a place
Dry needling is more precise. A thin needle goes into the trigger point to provoke a response in the muscle. In the right case, it can reach tissue that's hard to release with fingers alone. It's often a strong option when a patient says, “Massage helps for a day, then everything tightens back up.”
It isn't for everyone. Some patients dislike needles, bruise easily, or respond better to a slower manual approach. But when a trigger point is persistent and clearly reproducible, needling can be a good next step. For a deeper look at that method, this page on dry needling in physical therapy explains the clinical approach clearly.
Practical rule: The best technique is the one that changes pain and movement without unnecessarily irritating the tissue.
Injections and other advanced tools
Trigger point injections belong in the escalation conversation, not the starting point for every sore muscle. They can be helpful when a patient has gone through appropriate conservative care and still has a clear, stubborn pain generator. The same goes for other advanced modalities. They can be excellent in the right scenario, but they're not magic.
The common mistake is choosing the most aggressive option too early, or staying with a mild option too long after progress has stalled. Good care sits in the middle. It starts conservatively, reassesses objectively, and changes course when the tissue and symptoms say it's time.
How to Safely Perform Self-Care for Trigger Points
Home care helps. Bad home care sets people back.
That's the part many online guides skip. Self-release can maintain progress, but improper technique can aggravate symptoms, and research discussed in this review of trigger point therapy self-care notes that a significant percentage of patients report short-term worsening with unsupervised attempts. The biggest problem isn't the tool. It's using too much pressure, staying too long, or working on the wrong area.
Before you start, use this simple rule: aim for a tolerable, productive pressure, not a test of willpower. Many clinicians teach a “good pain” range around a 5 to 7 pain scale during home work, then back off if symptoms sharpen or linger.
A safe self-care routine
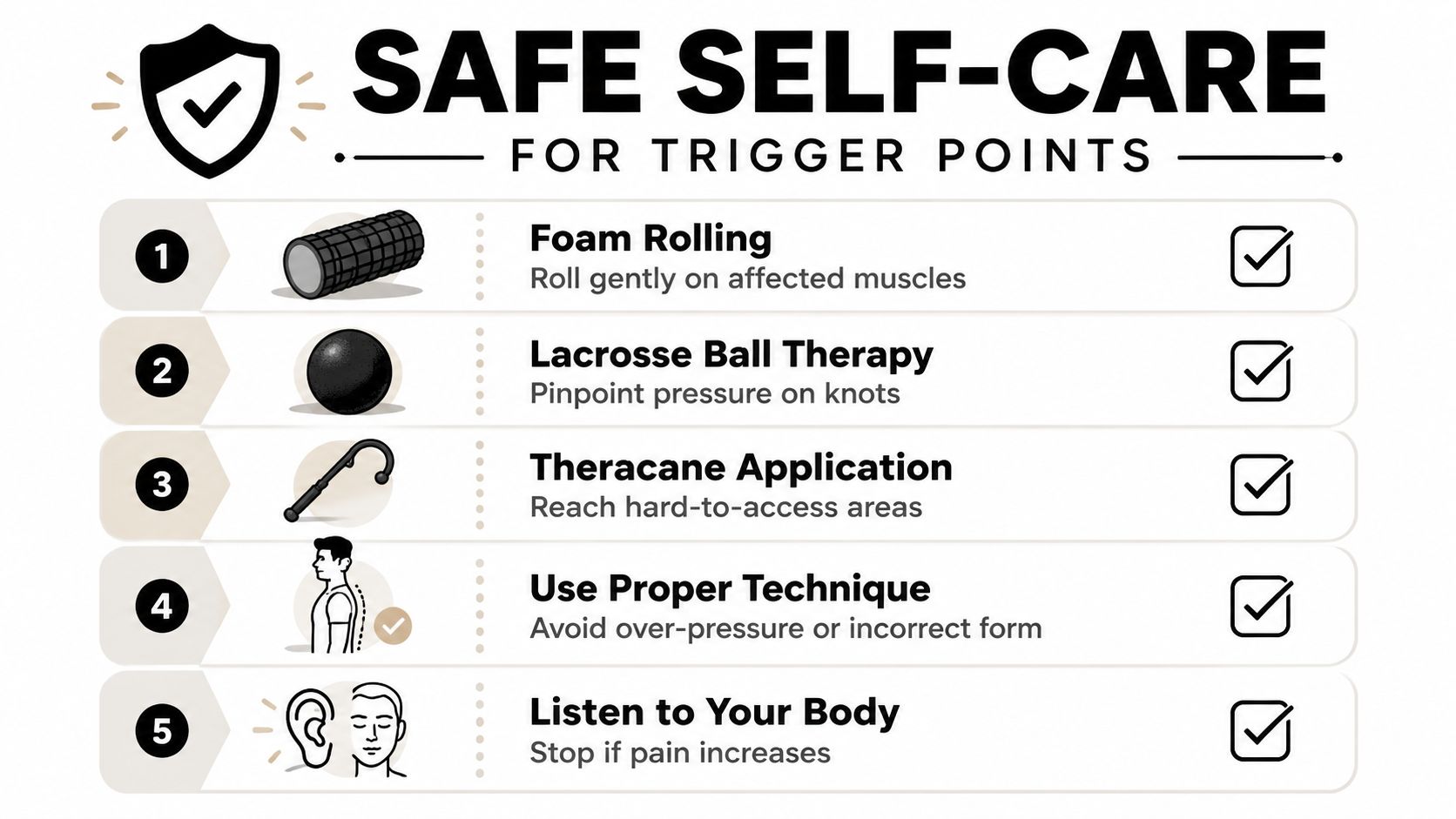
Choose one tool, not three.
Start with a foam roller for broad areas like the upper back, quads, or glutes. Use a lacrosse ball or Theracane only when you can clearly localize the painful spot.Set pressure gradually.
Lean into the tool until you feel firm discomfort, not a sharp or electric pain. If you're holding your breath or bracing your whole body, the pressure is too high.Stay on the point briefly.
Hold steady pressure, then ease off once the tenderness starts to soften. Don't grind aggressively over the spot.Recheck your movement right away.
Turn your head, raise your arm, or stand and walk. If movement is easier, you likely hit the right area with the right amount of pressure.Stop if symptoms spread the wrong way.
Some referral is expected when you contact a trigger point. What you don't want is rising pain, muscle guarding, numbness, or symptoms that keep building after you finish.
For broad muscle work at home, a PE foam roller can be useful because it gives more surface area and less pinpoint pressure than a hard ball.
Tool choice matters by body region
Neck and upper shoulder
A Theracane or ball against the wall is often better than lying directly on a hard ball. Control matters more than intensity. If neck pain is tied to poor sleep posture, a guide to choosing a cervical pillow for neck pain can help reduce the overnight strain that keeps reactivating the same trigger points.Mid back and shoulder blade area
A ball against the wall gives you precision without trapping you on the floor. Avoid jamming directly onto the shoulder blade itself.Glutes and hip
A lacrosse ball can work well here because the tissue is thicker. Sit on the ball, shift slowly, and avoid rolling fast.
This demonstration can help you visualize safe setup and pacing at home.
What doesn't work well
A few habits cause trouble quickly:
- Over-treating the same spot until it feels bruised
- Stretching aggressively first when the muscle is still highly irritable
- Using sharp pain as a guide instead of controlled pressure
- Buying harder tools when the issue is poor technique, not weak equipment
If self-care leaves you feeling worse for the rest of the day, that session was too much, even if it felt productive in the moment.
Your First Trigger Point Therapy Session
A first session usually starts with a conversation that's more specific than patients expect. Where is the pain? Where does it travel? What movements bring it on? What time of day is it worst? Those answers help separate a trigger point problem from joint irritation, nerve involvement, or a more complex pain pattern.
Then comes movement testing. A therapist might check neck rotation, shoulder elevation, spinal motion, gait, or how you transition from sitting to standing. That part matters because the painful muscle is not always the root driver. Sometimes the trigger point is reacting to weak support, poor mechanics, or a protective pattern that started after another injury.
What the hands-on work feels like
Once the point is identified, the therapist applies sustained digital pressure to the spot. The key neuromuscular principle is straightforward. Holding pressure for about 30 to 90 seconds can mechanically release tension in the muscle fibers, allow them to lengthen, and reduce local tenderness and referred pain, as explained in this guide to the mechanics of trigger point therapy.
At first, patients often feel a deep ache that they immediately recognize. Then the sensation changes. It may spread, pulse, soften, or feel like the tissue is melting under the pressure. Some areas twitch. Some let go in stages.
What happens after the treatment
Immediately, two outcomes are common: either improved movement right away, or initial soreness followed by greater looseness later that day or the next morning. Mild post-treatment soreness can be normal. What you want overall is easier movement, less familiar pain, and less resistance when you turn, reach, bend, or walk.
A good first visit also includes a plan. Not a vague “come back and we'll see,” but a practical next step. That may mean hydration, lighter activity for the rest of the day, one home release drill, or holding off on stretching until the muscle settles.
The first session should leave you with more clarity than confusion. You should understand what was found, what was treated, and what response to watch for next.
When to Consider Advanced Treatment Options
Manual trigger point therapy is useful, but there's a point where continuing the same approach becomes inefficient. If pain relief is brief, the trigger point never really softens, or progress stalls despite good compliance, it's worth asking whether conservative care alone is enough.
Patient education often stops too early. Data summarized in this review of persistent trigger point care and escalation suggests that trigger point injections have the most scientific support for persistent cases, and about 30% of chronic pain cases may require escalation beyond conservative manual therapy to resolve.
Signs that conservative care may be plateauing
Some patterns deserve a more direct conversation with your therapist or physician:
- Relief fades quickly and each session seems to reset the same pain without lasting change
- The trigger point remains highly irritable even when pressure is graded appropriately
- Function is still limited despite consistent treatment and home care
- Needling or manual release fails to produce meaningful tissue change, especially when the clinical response is flat over time
One clinical clue sometimes discussed in persistent cases is the absence of expected tissue response during treatment. That doesn't make one session a failure. It does tell us to stop assuming more of the same will eventually solve it.
Escalation is not giving up
Patients sometimes hear “advanced treatment” and think it means their body is worse than expected. Usually it means the plan is getting more precise. Injections, dry needling, or a broader medical workup can be appropriate when the pain generator is stubborn or the surrounding nervous system has become highly sensitized.
Staying too long with a failing approach has a cost. It delays recovery, reinforces fear, and often makes people distrust treatment that could still help if the strategy changes.
When to pause and reassess first
Trigger point therapy should also be reconsidered when symptoms don't behave like muscle pain. If pain is constant and unchanging, accompanied by unusual neurological symptoms, or clearly worsening without a mechanical pattern, the right next step may be medical evaluation before more hands-on work.
That balanced decision is part of good care. Not every painful spot needs stronger treatment. Some need a different diagnosis.
Your Path to Recovery at MedAmerica Rehab Center
Good trigger point care works best when it sits inside a bigger plan. A patient with desk-related neck pain may need manual release, posture retraining, and targeted exercise. An athlete may respond best to a combination of soft tissue work, progressive loading, and modality support. A senior with chronic stiffness may need a gentler pace, plus balance and gait work so the gains carry over into daily life.
That's where a multidisciplinary setting can help. Physical therapy, chiropractic care, acupuncture, and advanced modalities each bring a different lens. Used together, they can create a plan that is more individualized than any one technique alone.

What personalized care looks like
A few examples show how different that can look in practice:
For active adults
The plan may focus on releasing the trigger point, restoring joint motion, and correcting the training or movement pattern that overloaded the muscle in the first place.For post-accident patients
Treatment often needs a slower ramp-up. Guarding, pain sensitivity, and fear of movement can all make the muscles feel “stuck” long after the initial event.For older adults
The goal isn't just to press on sore spots. It's to reduce pain while improving confidence, stability, and day-to-day mobility.
Patients often benefit from seeing how wellness-focused providers present care philosophy and recovery environments. A good example is the Healhaus listing on Lucidoura, which shows how thoughtful, patient-centered healing spaces communicate support and intention.
The most important takeaway is simple. Trigger point therapy can be powerful, but it works best when it's matched to the problem, adjusted when progress stalls, and supported by the right home routine and movement plan.
If you're dealing with neck pain, back pain, sciatica, headaches, or stubborn muscle tightness that keeps returning, MedAmerica Rehab Center can help you figure out whether trigger point therapy is the right fit and what the next step should be if it isn't. Their Deerfield Beach team offers patient-centered physical therapy, chiropractic care, acupuncture, and advanced rehab options designed around your specific goals, not a generic protocol.