Iontophoresis Patch Dexamethasone for Effective Pain Relief
A lot of people arrive with the same story. One spot hurts every time they grip, reach, push off, or take that first step in the morning. They’ve already tried resting it, icing it, changing activities, and maybe taking an anti-inflammatory pill, but the pain keeps coming back.
It might be an irritated elbow after tennis, a stubborn Achilles tendon, a sore shoulder, or a foot that protests the moment they get out of bed. What they want is simple. They want relief aimed at the problem area, not a treatment that affects the whole body, and not necessarily a needle.
That’s where iontophoresis patch dexamethasone often enters the conversation. It’s a way to move anti-inflammatory medicine through the skin using a gentle electrical current. For many patients, that sounds unusual at first. Once you understand what happens during treatment and why therapists use it, it becomes much less mysterious.
When Localized Pain Just Won’t Go Away
You may know this feeling well. The pain isn’t everywhere. It’s in one maddeningly specific place.
You lift a grocery bag and the outside of your elbow flares. You reach overhead and the front of your shoulder complains. You get up from bed and your heel reminds you that yesterday’s walk was too much.

The kind of pain that changes your day
This type of pain can look small from the outside, but it changes normal life fast.
A few common examples:
- Tennis elbow: Turning a doorknob, holding a coffee mug, or using a screwdriver can hurt. If that sounds familiar, this guide to tennis elbow pain relief may also help you understand why the irritation lingers.
- Plantar heel pain: The first steps in the morning feel sharp, then the area loosens a little, then tightens again later.
- Shoulder bursitis or tendon irritation: Reaching into a cabinet or fastening a seatbelt suddenly becomes a problem.
- Localized wrist or hand irritation: Typing, gripping, or lifting can trigger the same exact sore spot every day.
People often tell me the worst part isn’t just the pain. It’s the stop-and-start cycle. It calms down, then returns the moment they become active again.
Why patients ask about a needle-free option
Many adults don’t love the idea of injections. Some are fine with them and some would rather avoid them if there’s a reasonable alternative.
That’s why iontophoresis gets attention. It offers a targeted, non-invasive way to deliver dexamethasone, an anti-inflammatory medication, toward the irritated tissue under the skin. Instead of swallowing medication that circulates through your whole system, the treatment focuses on a smaller area.
Some patients describe it as a middle ground between a cream and an injection. It’s more targeted than a rub-on product, but it doesn’t involve a needle.
That doesn’t mean it’s the right answer for every painful condition. It works best when the pain has a strong local inflammatory component and when your therapist can clearly identify the treatment area.
If you’ve been wondering what this treatment feels like, whether it’s safe, and what happens during the appointment, those are exactly the questions that matter.
How Iontophoresis Delivers Medicine Without Needles
The short version is this. Iontophoresis patch dexamethasone uses a mild direct electrical current to help move medication through the skin.
That sounds technical, but the basic idea is straightforward.
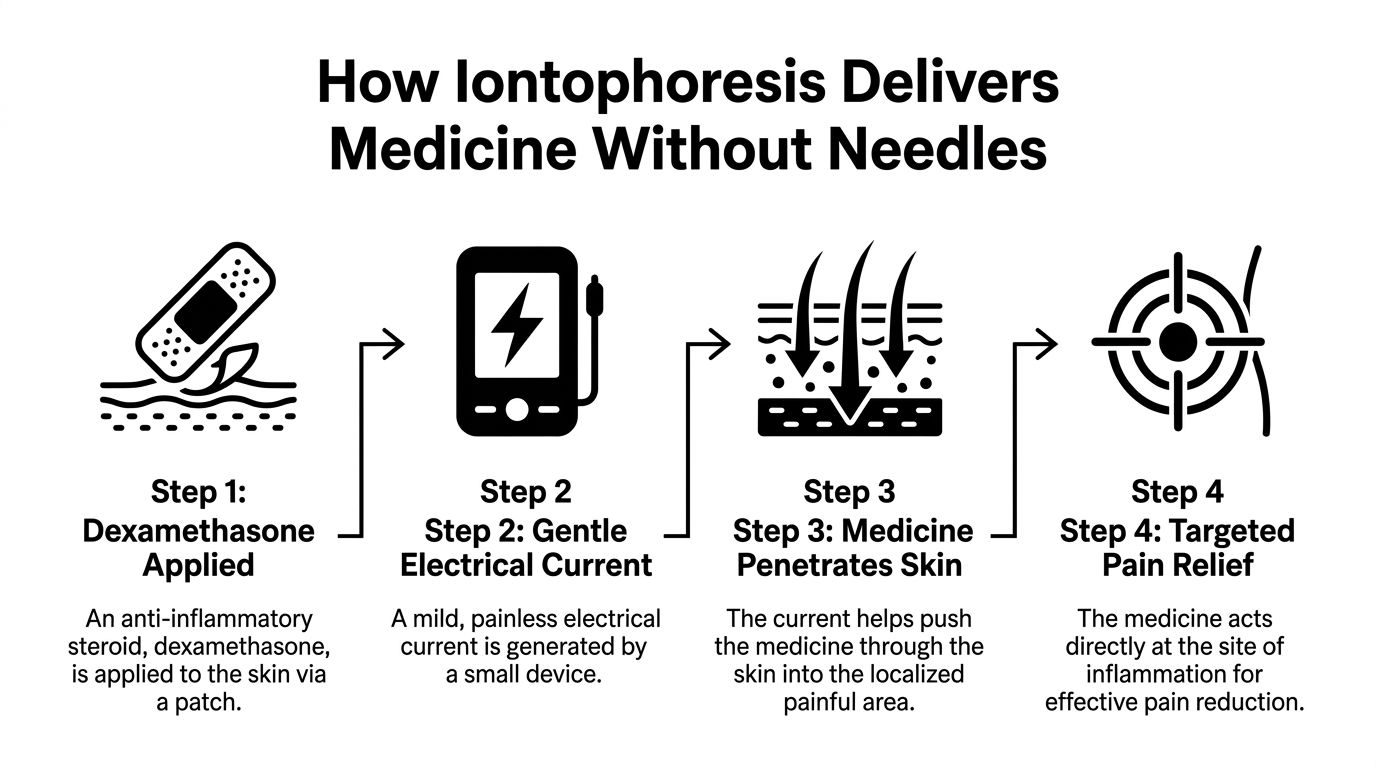
Start with the medicine
Dexamethasone is a corticosteroid medication used to calm inflammation. In physical therapy, it’s often chosen when a tendon, bursa, or other soft tissue structure is irritated and painful.
The goal isn’t to numb the body. The goal is to bring anti-inflammatory medication into a focused area.
The simple physics behind it
Dexamethasone used for iontophoresis is negatively charged. The patch system places that medicine under the negative electrode, also called the cathode.
Because like charges repel, the electrical current helps push the medication away from that negative side and into the skin. A plain-language explanation of this mechanism appears in the IontoPatch overview of how iontophoresis works, which notes that iontophoresis patches deliver dexamethasone with a low-level direct current, typically 1.0 to 4.0 mA, and that maximum safe current densities of 0.5 mA/cm² help protect the skin.
A useful analogy is a crowd at a doorway. If people behind you gently press forward, you move through the opening. The current gives the medication that gentle push.
Where the medicine goes
The skin isn’t one solid wall. Medicine can move through openings and less-resistant pathways, including sweat ducts, hair follicles, sebaceous glands, and tiny imperfections in the outer skin layer.
That’s why iontophoresis can help the medication reach tissue a few millimeters below the surface, where irritated tendons and connective tissues often live.
What it feels like
Iontophoresis is not typically described as painful.
They may feel:
- A mild tingling sensation
- A faint warmth
- A light prickly feeling at the pad
- Very little at all
If the sensation feels sharp or burning, the treatment settings or pad contact may need adjustment. That’s one reason proper setup matters.
Practical rule: You should feel that the treatment is on. You should not feel like you need to endure it.
How it differs from TENS
This is a common point of confusion.
A TENS unit uses electrical stimulation to help change how pain signals are perceived. It does not deliver medication through the skin.
Iontophoresis is different because the current has a delivery job. It helps move dexamethasone into the target area.
Here’s the easiest way to separate them:
| Device | Main purpose | Medication involved |
|---|---|---|
| TENS | Modulate pain signals | No |
| Iontophoresis | Deliver charged medicine through the skin | Yes, dexamethasone |
Why patients often like this idea
The appeal is easy to understand.
- It’s localized: Treatment focuses on the painful area.
- It’s needle-free: No injection into the tissue.
- It’s practical: Sessions can fit into a therapy plan.
- It’s familiar to rehab clinics: Therapists use it as one tool among several, not as a magic fix.
The patch isn’t doing something mysterious. It’s combining medication and controlled electrical current to create a targeted delivery system.
Is This Treatment Right for Your Condition?
Iontophoresis works best when your pain comes from a localized inflammatory problem rather than a broad, whole-body issue.
That distinction matters. If one small area is irritated, a targeted treatment makes sense. If symptoms come from several causes at once, your therapist may use iontophoresis as only one part of the plan, or skip it entirely.
Conditions that often fit the best
Here are the types of problems where therapists commonly consider iontophoresis patch dexamethasone.
Tendon irritation
This includes issues like tennis elbow, patellar tendon pain, Achilles irritation, and some rotator cuff tendon problems.
Why it fits: tendons often get irritated in a very specific spot. A targeted anti-inflammatory approach may help calm that area while exercise and activity changes address the underlying mechanical cause.
Bursitis
Bursae are small fluid-filled sacs that reduce friction around joints. When one gets irritated, the pain is often well localized.
Examples include some forms of shoulder bursitis and hip bursitis.
Why it fits: the irritated tissue is close enough to the surface that local treatment can make practical sense.
Joint-related inflammatory pain
Some joint conditions have a more inflammatory component than others.
A clinical review discussing dexamethasone iontophoresis reported that, in a pilot study of temporomandibular joint arthritis, jaw opening improved in 68% of cases and pain resolved in 73% (PMCID article on dexamethasone iontophoresis). The same review also described pain reduction after activity in patellar tendinopathy, which supports its use in certain joint and tendon problems.
Carpal tunnel and similar overuse conditions
This is a more selective area. Some clinicians try iontophoresis when inflammation appears to be contributing to symptoms, but results can be mixed.
That’s an important point. A treatment can be useful without being universal.
When it may be less helpful
Some painful conditions don’t respond as well because inflammation isn’t the main driver, or because the painful tissue sits too deep, or because the diagnosis is more complex than it first appears.
You may need a different plan if your symptoms are mostly related to:
- Nerve compression without clear local inflammation
- Pain referred from the neck or low back
- Widespread arthritis affecting many joints
- Major strength or movement deficits that need exercise first
- Skin sensitivity or medical contraindications
A better question than does it work
Patients often ask, “Does iontophoresis work?”
A better question is, “Does it fit my diagnosis?”
That’s what a good evaluation tries to answer. Two people can both say, “My shoulder hurts,” and need very different care.
The treatment is strongest when the problem is specific, the painful tissue is identifiable, and the rehab plan also addresses why that tissue got overloaded in the first place.
The patients who usually do best
In day-to-day rehab, the best candidates often share a few traits:
- Their pain is localized: They can point to one small region.
- Their symptoms are reproducible: The same movement triggers the same area.
- Inflammation seems active: There’s tenderness, soreness after use, or irritation that hasn’t settled.
- They want to avoid an injection if possible: A patch-based option feels more approachable.
- They’re open to combined care: They understand the patch helps calm tissue, while therapy helps restore movement and load tolerance.
That combination matters. Iontophoresis isn’t a replacement for rehab. It’s a way to make rehab more tolerable and, in the right case, more effective.
What the Research Says About Iontophoresis Effectiveness
Patients usually want one honest answer. Is this treatment backed by real evidence, or is it just one more gadget?
The useful answer is that research supports iontophoresis as a real drug-delivery method, and some studies show meaningful symptom improvement in selected conditions. At the same time, the evidence is stronger for short-term outcomes than for long-term promises.
The key question researchers studied
One major question was simple. Does dexamethasone get into human tissue with iontophoresis?
A 2015 pharmacokinetic study answered that directly. It found that iontophoresis delivered dexamethasone into human tissues, that tissue levels exceeded the median effective dose (ED50) during treatment, and that local skin perfusion increased by over 700% during treatment (2015 pharmacokinetic study).
That matters because it shows the treatment isn’t just creating a sensation on the skin. It’s producing measurable biological effects.
What that means for a patient
If I translate that into everyday language, it means this:
- The medicine can be moved through the skin into tissue.
- The treated area shows a strong local physiological response.
- The approach has a scientific basis, not just anecdotal use.
That doesn’t guarantee every painful elbow, heel, or shoulder will improve. It does support the idea that the delivery method is legitimate.
Clinical improvement in real conditions
Other clinical work adds a more practical layer. Some studies report reduced pain after activity, improved function, or better motion in specific diagnoses.
That’s the kind of information patients care about most. Not just “did the medicine get there,” but “did people move better afterward?”
If you like reading patient-friendly materials before trying a treatment, this collection of Top Patient Education Resources can help you compare how different rehab topics are explained across trusted health content.
A balanced view matters
Research on iontophoresis is encouraging, but it isn’t a blank check.
Here’s the balanced takeaway:
| What research supports | What still needs caution |
|---|---|
| Dexamethasone can be delivered through the skin into human tissue | Not every condition responds equally well |
| Short-term symptom improvement is reported in some diagnoses | Long-term benefit is less certain for some problems |
| The treatment has measurable local effects | It should be chosen based on diagnosis, not as a routine add-on |
Good evidence doesn’t mean “works for everyone.” It means the treatment has a clear rationale, measurable effects, and a sensible place in care when the diagnosis fits.
For most patients, that’s the right way to think about it. Not miracle treatment. Not gimmick. A useful, evidence-based option when used thoughtfully.
What to Expect During Your Treatment Session
The first thing most patients want to know is whether the appointment will feel strange. In practice, it’s usually much more ordinary than they expect.
A typical visit starts with a therapist confirming that the painful area, your symptoms, and your overall rehab plan make iontophoresis worth using.

Before the patch goes on
Your therapist usually checks a few things first:
- The exact pain location: A treatment like this works best when the irritated tissue can be identified clearly.
- Your skin: The area should be intact, not scraped, broken, or highly irritated.
- Your medical history: This helps rule out reasons to avoid the treatment.
- Your movement pattern: The patch may calm symptoms, but your therapist also needs to know what keeps provoking them.
If you’ve never been to PT before, this overview of what a typical physical therapy session looks like gives a helpful picture of how an appointment is structured.
What the setup looks like
The skin is cleaned first so the electrodes sit well and the current flows evenly.
Then the treatment pads are placed:
- One pad contains the dexamethasone solution.
- The other pad completes the circuit, often using saline.
- The device is turned on and adjusted to a comfortable level.
You don’t need to “do” anything special during this time. Typically, individuals sit comfortably and relax.
Wired session or wireless patch
There are two common ways this treatment is delivered.
In-clinic wired treatment
A traditional setup delivers a therapeutic dose of 40 to 80 mA·min over a 20 to 40 minute clinic session. Rehab education on iontophoresis parameters also notes that this is often done 3 to 5 times per week as part of a broader therapy plan, while wire-free systems can deliver the same dose over longer wear times such as 2.5 hours (clinical dosing overview).
This option is useful when the therapist wants to monitor the full session in real time.
Wireless patch
Some systems, such as IontoPatch or ActivaPatch, are designed so you can leave with the patch on while it continues delivering the dose over a longer period.
Patients often like this because it feels less disruptive. Instead of sitting attached to wires, they can continue with the rest of the day more normally, within the instructions they’re given.
What you may feel during treatment
Sensations vary, but common descriptions include:
- Gentle tingling
- A light prickly feel
- Mild warmth
- Temporary redness afterward
That redness usually reflects local skin response and often fades. If the area feels intensely irritated, your therapist should know right away.
The sensation should be tolerable and predictable. If it feels aggressive, the setup needs attention.
A quick visual example can help if you’re a person who likes to see equipment before trying it:
What happens after the patch
The session rarely ends with the patch alone.
Your therapist may pair it with:
- Gentle mobility work
- Targeted strengthening
- Load management advice
- Stretching when appropriate
- Home instructions for the next 24 hours
That combined approach matters because the medication may calm the area, but your body still needs to relearn how to tolerate movement and load.
A practical example: if your elbow pain flares every time you grip, the patch may help reduce irritation, while your exercise plan improves tendon tolerance so the same tasks stop triggering the problem.
Understanding the Risks and Your Other Options
A good treatment conversation should include the benefits, the limits, and the alternatives.
Iontophoresis is generally considered well tolerated in the short term, but that doesn’t mean it’s for everyone.
When iontophoresis may not be appropriate
Your clinician may avoid this treatment if you have:
- Broken or irritated skin where the electrodes would go
- A known sensitivity to the medication or adhesive
- A pacemaker or certain implanted electrical devices
- A condition where another treatment better matches the diagnosis
These decisions should be individualized. The right choice depends on the tissue involved, your symptoms, and your full medical picture.
The main risks patients should know
The most common risks are skin-related.
A systematic review summary notes that short-term studies generally show iontophoresis is well tolerated, that long-term efficacy data is more limited for some conditions such as epicondylitis, and that known risks are mainly skin irritation or, more rarely, small burns if protocols aren’t followed correctly (systematic review summary on PubMed).
That’s why professional supervision matters. Good skin prep, correct electrode placement, and proper dosing reduce avoidable problems.
Treatment Comparison Iontophoresis vs. Other Options
| Treatment | How It Works | Pros | Cons |
|---|---|---|---|
| Iontophoresis | Uses mild electrical current to move dexamethasone through the skin into a local area | Needle-free, targeted, often well tolerated, fits into rehab sessions | Skin irritation can occur, not ideal for every diagnosis, long-term benefit may be limited in some conditions |
| Corticosteroid injection | Delivers anti-inflammatory medicine by needle into or near the painful area | Direct delivery, often familiar to patients and physicians | Invasive, needle-based, may not be the preferred first option for every patient |
| Oral anti-inflammatory medication | Reduces inflammation systemically after swallowing medication | Convenient, widely available | Less targeted, affects the whole body rather than one specific tissue |
| Shockwave therapy | Uses acoustic energy to stimulate tissue response | Non-surgical option used for selected musculoskeletal problems | Not the same mechanism, may be better for some diagnoses and less relevant for others |
Another non-surgical option some patients ask about is shockwave therapy for pain relief and recovery. It works very differently from iontophoresis, so the better choice depends on the tissue problem, not which treatment sounds newer.
A smart rehab plan doesn’t force one treatment onto every diagnosis. It matches the tool to the problem.
The honest bottom line on safety
If your pain is localized and your skin is healthy, iontophoresis is often a reasonable treatment to consider. If your symptoms are widespread, your diagnosis is unclear, or your skin is sensitive, another approach may make more sense.
The best version of care is not “always choose the patch.” It’s “choose the treatment that fits.”
Your Questions About Iontophoresis Answered
Patients usually ask the practical questions last, but these are often the ones that determine whether treatment feels manageable.
How many treatments will I need
There isn’t one universal answer.
Some people try a short series and then reassess. In many rehab settings, iontophoresis is used for a limited run while the therapist watches for changes in pain, tenderness, and function.
If you aren’t noticing any meaningful change after a reasonable trial, your therapist should reconsider the plan instead of repeating the same thing endlessly.
Does it hurt
Usually, no. It is commonly described as mild tingling, mild warmth, or a light prickly sensation.
If it stings, burns, or feels stronger than expected, tell your clinician. The goal is therapeutic dosing, not discomfort.
Can I do this myself at home
Not in the same way a clinician does it from scratch.
Some wireless patches are designed for extended wear, but the decision to use them, the medication setup, the dosing, and the skin checks should come from a licensed professional. This isn’t the kind of treatment you want to improvise.
Is it covered by insurance
Coverage depends on your plan, diagnosis, and clinic billing rules.
The most useful step is to ask the clinic staff to verify benefits before treatment starts. That avoids surprises and helps you compare options.
Can it be combined with other approaches
Yes, often.
That may include exercise therapy, manual therapy, activity modification, and sometimes broader self-care strategies. For patients with arthritis or general joint discomfort, some also explore nutrition support and read about supplements for joint pain alongside their rehab plan. Supplements don’t replace diagnosis or treatment, but patients often appreciate understanding the full scope of options.
When should I see a clinician instead of waiting it out
You should get checked if the pain is:
- Lasting longer than expected
- Returning every time you resume activity
- Interfering with sleep, work, or walking
- Getting worse instead of better
- Paired with weakness, numbness, or major stiffness
Localized pain often starts as an annoyance. Then people adapt around it for weeks or months. By that point, the tissue may be more irritable and your movement patterns may already be compensating.
That’s why earlier assessment can help. Sometimes the patch is useful. Sometimes it isn’t. The value is in getting the diagnosis right and building a plan that matches your body, your goals, and your daily life.
If you’re dealing with stubborn, localized pain and want a clear plan instead of guesswork, MedAmerica Rehab Center can help you figure out whether iontophoresis patch dexamethasone fits your condition. Their team provides patient-centered rehab for pain relief, mobility, and recovery, with treatment plans built around what you need to get back to doing comfortably.