Physical Therapy for Shoulder Injury in Deerfield Beach
Reaching into the back seat hurts. Lifting a pan out of the oven hurts. Even sleeping on one side starts waking you up at night.
That pattern is common with shoulder problems, but it isn't something you should just accept and work around forever. A sore shoulder often starts as an annoyance, then slowly changes how you dress, drive, exercise, work, and rest. Many people don't notice how much they've adapted until simple tasks feel awkward.
Physical therapy for shoulder injury gives you a structured way to stop guessing. Instead of bouncing between rest, random stretches, and “trying not to use it,” you get a plan built around how your shoulder moves, what tissue is irritated, and what activities you need to get back to. At MedAmerica Rehab Center in Deerfield Beach, that process also includes practical coordination around care operations when needed. For clinics trying to streamline related documentation and payment workflows around hands-on services, Fitness GM's medical massage billing solution is one example of the kind of operational resource that supports smoother patient care behind the scenes.
That Nagging Shoulder Pain Is Not Normal
A lot of shoulder injuries don't begin with one dramatic moment. They develop gradually. You reach into a cabinet and feel a pinch. You carry groceries and notice weakness. You put on a shirt and your arm doesn't want to move the way it used to.
Then the compensations begin.
You start using the other arm more. You stop lifting overhead. You avoid workouts that used to feel easy. At night, you shift around trying to find one position that doesn't ache. That's usually the point when people realize this isn't just “sleeping on it wrong.”
What shoulder pain often disrupts first
- Overhead reaching: Getting dishes, hair care, dressing, and housework become irritating fast.
- Carrying and lifting: Bags, laundry baskets, and children often expose weakness before anything else does.
- Sleep: A shoulder that hurts at rest usually gets your attention quickly.
- Work tasks: Desk setup, driving, repeated reaching, and manual labor can all keep symptoms going.
Physical therapy for shoulder injury is useful because it turns that frustrating experience into a sequence you can follow. A therapist looks at pain, motion, strength, posture, and movement quality together. That matters, because the shoulder rarely acts alone. The shoulder blade, upper back, rib cage, neck, and rotator cuff all influence how that joint handles load.
Practical rule: If shoulder pain keeps changing how you move through the day, it deserves more than rest and hope.
Patients don't need another generic exercise list. They need a realistic path. That includes what to do first, what improvement should look like, and what to do if things aren't progressing the way they should.
Understanding Your Shoulder Anatomy and Injury
The shoulder is a ball-and-socket joint, but that simple label hides how much coordination it needs. A better way to think about it is this: the ball is large, the socket is relatively shallow, and the whole system depends on a group of smaller structures keeping everything centered while you move.
The parts that matter most
Three bones form the basic framework:
- Humerus: the upper arm bone
- Scapula: the shoulder blade
- Clavicle: the collarbone
Around them sits the support team.
The rotator cuff is a group of four muscles that helps hold the ball of the upper arm in the socket while you lift, reach, rotate, and lower the arm. If those muscles are weak, irritated, or poorly coordinated, the shoulder can feel painful, unstable, or easily fatigued.
The labrum is a rim of tissue that deepens the socket. Think of it as the edge that helps the ball sit more securely. The bursa is a fluid-filled cushion that helps tissues glide with less friction. When that area gets irritated, movement can feel sharp or pinchy.
For patients dealing with painful overhead motion, this overview of rehabilitation for shoulder impingement shows how anatomy and mechanics often overlap in real treatment.
Why common shoulder injuries hurt the way they do
Different diagnoses can create similar symptoms, which is why evaluation matters.
| Condition | What's often happening | What it may feel like |
|---|---|---|
| Impingement | Tissues get compressed during certain arm motions | Pinching with reaching or lifting overhead |
| Rotator cuff irritation or tear | Tendons struggle to tolerate load or are structurally injured | Pain, weakness, trouble lifting or lowering the arm |
| Bursitis | The cushioning tissue becomes inflamed | Aching, tenderness, pain with repetitive movement |
| Adhesive capsulitis | The joint becomes stiff and resistant in multiple directions | Marked stiffness, limited reach, painful motion |
The shoulder is mobile by design
The shoulder has to trade some stability for freedom of movement. That's why it can place your hand overhead, behind your back, and across your body. The downside is that if one part of the system stops doing its job, another part usually takes on too much stress.
A painful shoulder isn't always a “bad shoulder.” Often it's a shoulder that has lost timing, control, or load tolerance.
That's also why successful rehab usually isn't about one magic stretch. It's about restoring how the whole system works together.
The Pillars of Modern Shoulder Physical Therapy
Good rehab doesn't chase symptoms only. It identifies what the shoulder can't do well yet, then rebuilds it in the right order.
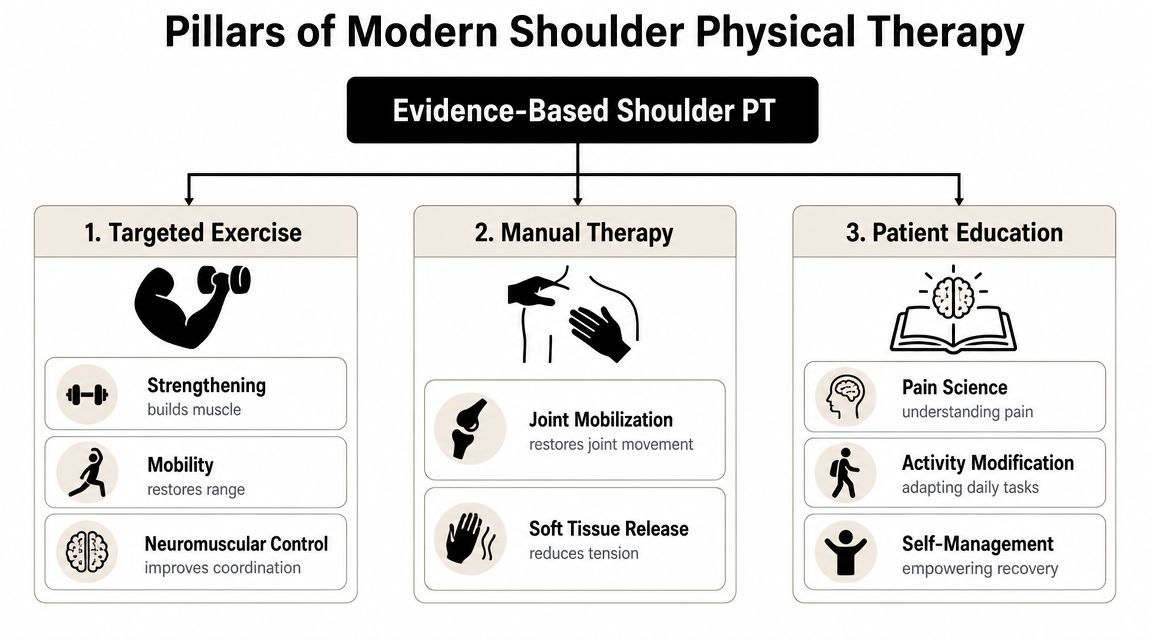
One reason modern care looks different from older “rest and modalities” plans is that the best programs focus on function. The principles are straightforward: shoulder rehab works better when treatment emphasizes progressive strengthening and improved motor control of the scapular and rotator cuff muscles, because those pieces address the biomechanical drivers of pain and function loss, as discussed in this review of the new gold standard in shoulder rehab.
Targeted exercise restores capacity
Exercise is the center of most shoulder rehab plans. Not random exercise. Specific exercise.
A therapist chooses movements based on what you're missing. Some people need early motion without aggravation. Others need cuff strength, scapular control, or better coordination during reaching. The progression matters as much as the exercise itself. Too easy and nothing changes. Too aggressive and symptoms flare.
When therapists measure motion, they often use tools such as a goniometer to track changes more objectively. If you want to understand that measurement process, this goniometer shoulder ROM guide gives a clear overview of how range of motion is assessed.
Manual therapy creates room to move
Hands-on care can help when the shoulder is too stiff, guarded, or painful to move well on its own. That may include joint mobilization, soft tissue work, or guided movement.
Manual therapy is rarely the entire answer, but it often makes exercise more effective. If lifting your arm is restricted because the joint is stiff or the surrounding muscles are overprotective, hands-on treatment can reduce that barrier enough for you to train the movement correctly.
One clinic option like MedAmerica Rehab Center may prove suitable. It offers physical therapy and a hands-on, drug-free approach for shoulder rehabilitation within a broader rehab setting.
After the shoulder calms down, patients often understand the process better when they can see movement and exercise examples in action.
Education and load management prevent the same cycle
Patients often think rehab is only exercise plus treatment table work. It isn't. Education changes outcomes because daily habits can keep re-irritating the shoulder.
That includes:
- Activity modification: Changing lifting angle, grip, or work setup so the shoulder isn't provoked all day
- Pain understanding: Knowing the difference between acceptable soreness and a true setback
- Home progression: Learning when to advance, when to hold steady, and when to speak up
The strongest rehab plan is one you understand well enough to follow outside the clinic.
Your First Visit What to Expect at MedAmerica
The first visit should reduce uncertainty, not add to it. Patients often come in wondering two things: What's wrong, and what will this take to fix?
The appointment usually starts with a conversation, not a workout. Your therapist wants the story first. Was the pain caused by a fall, repetitive strain, gym training, poor sleep, or a movement that suddenly felt wrong? Is it sharp, aching, weak, stiff, or inconsistent? Does it travel into the arm? Does it wake you up?
The questions matter
Those details help narrow the problem quickly. Shoulder pain from a stiff capsule behaves differently than pain from a cuff overload pattern or irritation that only appears overhead.
You'll also talk about what you need your shoulder to do. That might be tennis, golf, typing, carrying grandchildren, returning to work duties, or sleeping through the night. Goals shape treatment.
For patients who want a broader picture of how visits are typically structured, this overview of what a typical physical therapy session looks like helps set expectations.
The physical exam is practical
A shoulder evaluation usually includes:
- Range of motion testing: Can you lift, rotate, and reach without compensation?
- Strength testing: Which motions feel weak, painful, or unstable?
- Movement observation: Does the shoulder blade move well, or does the body substitute with shrugging and trunk leaning?
- Symptom reproduction: Which positions bring on the exact pain you've been feeling?
Therapists aren't just checking whether something hurts. They're looking for patterns. Sometimes pain appears because the shoulder is stiff. Other times it appears because the shoulder moves too freely without enough muscular control.
You should leave with a plan
By the end of the visit, the goal is clarity. You should understand the likely driver of your pain, what the early treatment priorities are, and what you'll be doing at home.
What patients usually need most: a simple explanation, a starting plan they can follow, and clear signs of whether recovery is moving in the right direction.
A good first visit also sets expectations. Shoulder recovery rarely follows a perfectly straight line. Some sessions focus on calming things down. Others focus on restoring movement or rebuilding strength. The plan changes as your shoulder changes.
A Sample Shoulder Rehab Timeline and Home Program
Recovery doesn't happen all at once. It usually moves through phases, and each phase has a different job. That's useful to know because many people get discouraged when they compare the wrong milestone to the wrong stage.
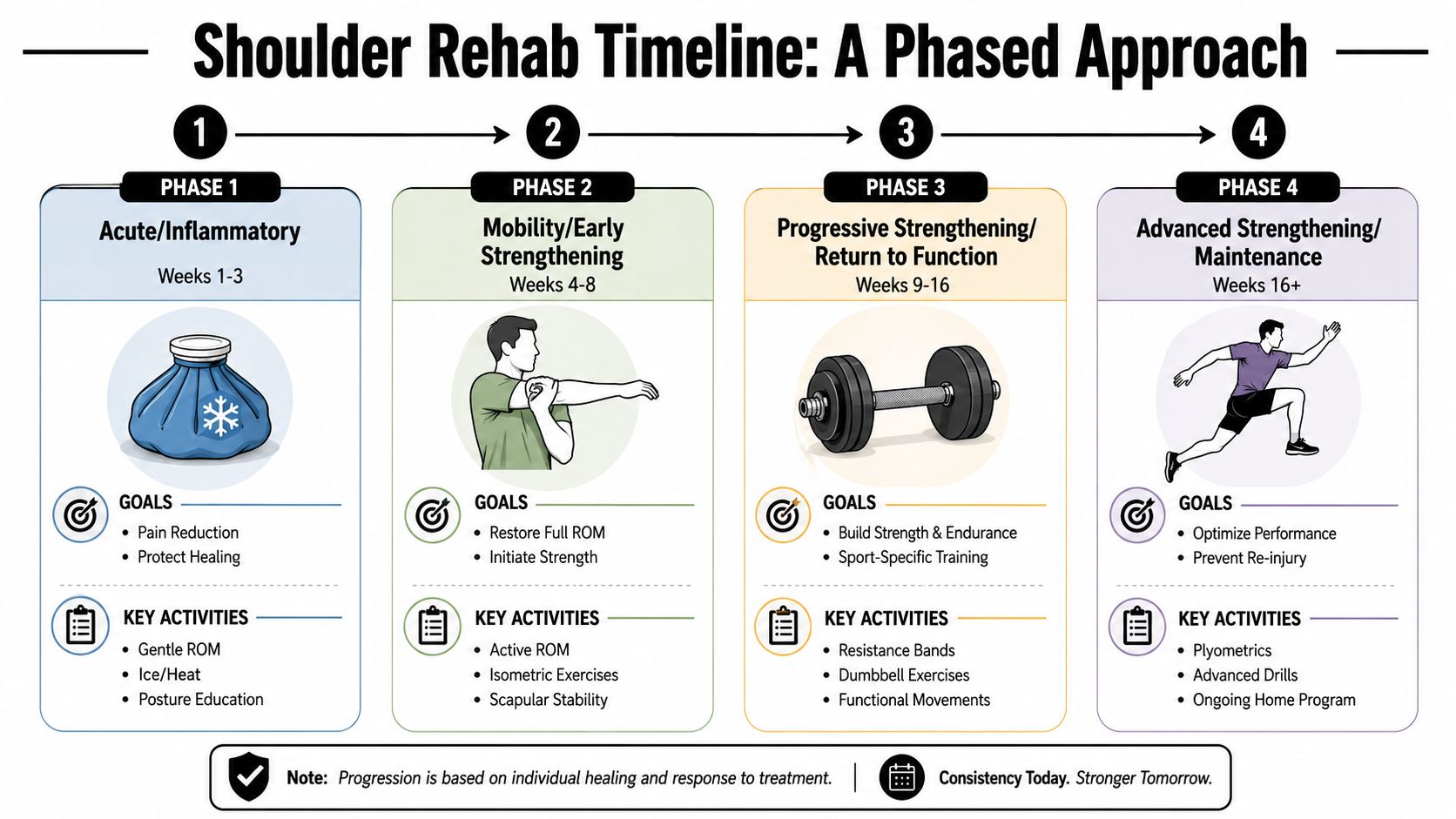
Early phase focuses on calming and moving
In the beginning, the main goals are reducing irritation and restoring tolerable motion. That may mean gentler drills, shorter ranges, and smarter use of the arm during daily tasks.
Common home work in this stage may include:
- Pendulum movements: Helpful when the shoulder needs motion without a lot of effort
- Table or wall slides: Useful for restoring assisted elevation
- Isometric contractions: Gentle muscle activation without large joint motion
- Posture resets: Simple positioning to reduce strain around the shoulder blade and neck
If a therapist wants you to add assisted range of motion work at home, a tool like an over-the-door pulley exerciser can be part of that stage when it fits the problem.
Middle phase builds control and strength
Once pain is more manageable and motion improves, rehab shifts toward load tolerance. At this point, many people start to feel hopeful, because the shoulder begins doing more instead of just hurting less.
Exercises may include band external rotation, scapular control drills, rowing patterns, and controlled reaching tasks. The emphasis is usually on quality. If the shoulder blade tips, shrugs, or wings every time you lift, the movement needs retraining before heavier loading makes sense.
A strong reason to stay consistent here is that structured exercise has measurable prevention value. A 2023 systematic review reported that the Shoulder Control programme performed three times weekly produced a 56% lower shoulder injury rate versus usual care, supporting the value of consistent, targeted rehab exercise in active populations (BMJ Open Sport & Exercise Medicine systematic review).
Late phase returns you to real life
The last phase is where rehab starts to look more like your actual goals. A golfer needs rotation control and repeated swing tolerance. A parent may need lifting endurance. A worker may need overhead capacity. A recreational athlete may need speed, confidence, and repeated effort.
Here's a simple way to think about the progression:
| Phase | Main priority | Example home emphasis |
|---|---|---|
| Early | Calm symptoms and restore safe motion | Pendulums, assisted motion, isometrics |
| Middle | Build strength and control | Bands, scapular drills, controlled lifting |
| Late | Return to task-specific activity | Endurance, higher load, sport or work patterns |
The timeline varies by diagnosis, age, irritability, and whether there's a more complex issue in the joint. What matters most is not rushing from one phase to the next before the shoulder is ready.
When to Be Concerned Red Flags in Your Recovery
A common mistake in shoulder rehab is assuming every increase in pain means you should “push through it.” That mindset can delay progress when the shoulder is telling you the plan needs adjustment.
Some soreness after exercise can be normal. A worsening pattern is different.
Signs that deserve a conversation quickly
These changes should prompt you to contact your therapist or referring provider:
- Pain is clearly escalating: not just temporary exercise soreness, but pain that stays high and disrupts sleep or basic use more than before
- You lose motion suddenly: reaching, rotating, or lifting becomes harder after it had been improving
- Strength drops off: the arm feels newly weak, shaky, or unable to manage familiar tasks
- New numbness or tingling appears: especially if symptoms extend further down the arm or feel neurologic rather than muscular
- The shoulder feels unstable: slipping, catching, or giving way is different from ordinary post-exercise fatigue
If your shoulder is getting harder to use week by week, that isn't a badge of effort. It's information.
When standard advice may not be enough
A major gap in patient education is knowing when to stop repeating the same routine and get checked again. Shoulder pain is often more complex than a simple strain. Rotator cuff tears, adhesive capsulitis, and overlapping impingement patterns can look similar at first but respond differently over time.
The American Academy of Orthopaedic Surgeons suggests continuing a shoulder exercise program for 4 to 6 weeks unless otherwise specified, which supports using a structured trial rather than endless self-management. If you're not making progress in that window, re-evaluation is reasonable (AAOS rotator cuff and shoulder conditioning program).
What happens next if progress stalls
Re-evaluation doesn't automatically mean surgery or a worst-case diagnosis. Often it means the plan needs to change.
That may include:
- Exercise modification: changing range, resistance, frequency, or movement selection
- Diagnosis review: reconsidering whether stiffness, tendon irritation, nerve involvement, or structural injury is the main issue
- Medical communication: updating your physician if symptoms suggest imaging or specialist input would be helpful
- Activity reset: removing one or two aggravating tasks that keep reloading the shoulder between visits
The key message is simple. Good rehab includes decision points. If your shoulder isn't improving, speaking up early is smarter than grinding through another month of the same pain.
Begin Your Recovery in Deerfield Beach Today
Shoulder recovery usually asks for more than rest, ice, and internet exercises. You need a plan that matches the actual problem, adapts when your symptoms change, and keeps you moving toward real goals.
That's especially true when the shoulder affects several parts of life at once. Work, sleep, exercise, driving, and basic home tasks all place different demands on the joint. A useful rehab plan connects those dots instead of treating the shoulder like an isolated part.
What practical care should look like
A solid clinic experience should give you:
- One-on-one evaluation: so the plan fits your movement pattern, not a generic diagnosis label
- Hands-on treatment when needed: especially when stiffness or guarding blocks progress
- Targeted exercise progression: from pain-limited movement to strength and daily function
- Clear next steps: including what to do if progress slows or symptoms change
MedAmerica Rehab Center has served Deerfield Beach since 1995 and provides physical therapy, chiropractic care, acupuncture, and shockwave therapy in one setting. For patients, that means shoulder care can stay coordinated instead of fragmented.
Getting started should be simple
Bring comfortable clothes, your insurance information, and any relevant imaging or referral paperwork you already have. Be ready to describe when the pain started, what makes it worse, and what you want to get back to doing.
Same-day appointments and insurance-friendly processes can make the first step easier, especially when pain is already interfering with daily life. The most important part is not waiting until the shoulder becomes your new normal.
If you're looking for physical therapy for shoulder injury in Deerfield Beach, start with an evaluation that gives you a clear picture of the problem and a realistic path forward.
If shoulder pain is limiting your sleep, work, workouts, or everyday movement, schedule an evaluation with MedAmerica Rehab Center. The team can assess how your shoulder is moving, explain what's likely driving the pain, and build a treatment plan that fits your goals and your daily life.