Pain Management Physical Therapy in Deerfield Beach
Some mornings, pain starts negotiating with you before your feet hit the floor. You sit up slowly to test your back. You angle your neck before checking your phone. You think about whether the grocery trip, the drive to work, or a walk on the beach is worth the flare-up later.
That kind of pain changes more than movement. It changes decisions, routines, sleep, mood, and confidence.
For many people in Deerfield Beach, the question isn't just, “How do I make this stop?” It's, “How do I get my life back?” That's where pain management physical therapy matters. Done well, it's not about chasing a miracle cure. It's about helping your body move better, helping your nervous system calm down, and helping you return to daily life with more control.
Beyond the Painkiller A New Approach to Feeling Better
A lot of people come to physical therapy after trying to push through pain for months. They've used rest, heat, over-the-counter medication, a brace they bought online, or stretches that felt good for a few minutes but didn't change much by the next day. Some were told to “wait and see.” Others were told pain was just part of getting older.
We see a different reality. Pain may be common, but living around it forever isn't the only option.
Pain management physical therapy gives you another path. Instead of only muting symptoms for a few hours, it looks at how you move, what loads your joints and muscles can handle, what your nerves are reacting to, and what daily tasks have become harder than they should be. That shift matters. It moves care from short-term coping toward long-term function.
Why PT is no longer a last resort
Physical therapy is firmly part of mainstream healthcare, not a fringe add-on. The U.S. Bureau of Labor Statistics reports that physical therapists help injured or ill people improve movement and manage pain, with a median annual wage of $101,020 in May 2024 and projected employment growth of 11% from 2024 to 2034, which equals about 13,200 openings per year on average according to the Bureau of Labor Statistics overview of physical therapists. That scale reflects how established PT has become across clinics, hospitals, home health, and nursing facilities.
The same BLS page notes the American Physical Therapy Association's point that the CDC recommends safe alternatives like physical therapy to manage most pain. In plain language, PT is often considered a first-line option, not something you try only after medication or surgery.
Practical rule: If pain is changing how you sit, sleep, walk, lift, or work, it's time to evaluate movement, not just symptoms.
What this looks like in real life
A person with back pain may not need stronger pain medicine. They may need to learn why standing from a chair hurts, why one side of the hip is overworking, or why the spine stiffens after long drives. Someone with neck pain and headaches may need better shoulder and upper-back control more than another pillow.
That's the promise of pain management physical therapy. Not false hope. Real progress.
Understanding Pain Management Physical Therapy
Pain management physical therapy is best understood as a problem-solving process. We don't just ask where it hurts. We ask what happens before it hurts, what movements trigger it, what positions calm it, how long it has been going on, and what the pain is stopping you from doing.
A good physical therapist works like a detective for your body. The painful area matters, but it's often only part of the story.
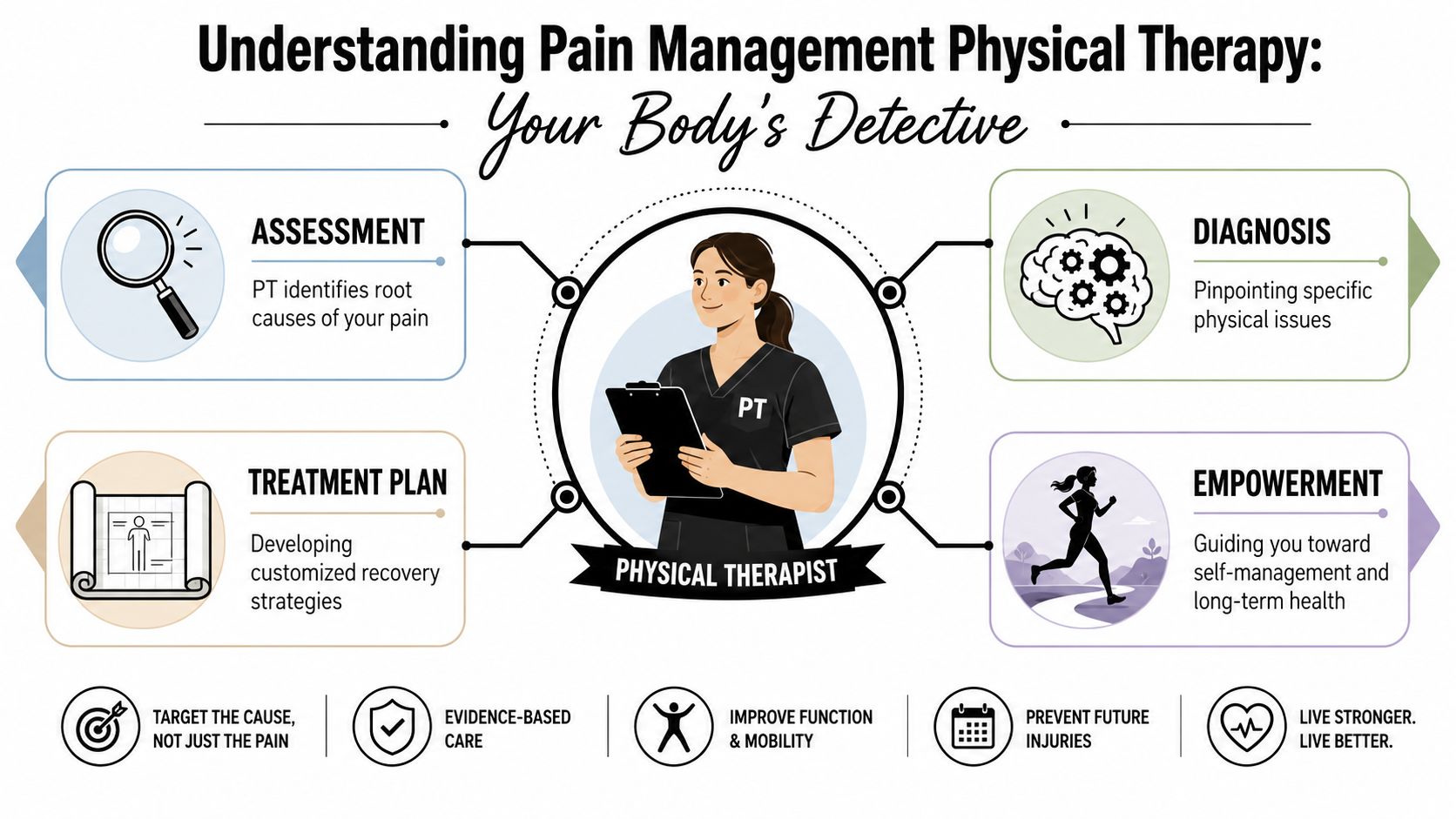
Looking past the pain spot
Take a simple example. Someone feels pain at the base of the neck every afternoon. A symptom-only approach says, “The neck hurts, so rub the neck.” A physical therapy approach asks more useful questions:
- Posture pattern: Are the head and shoulders drifting forward during computer work?
- Mobility issue: Is the upper back too stiff to support normal neck motion?
- Strength gap: Are the deep neck muscles and shoulder stabilizers underperforming?
- Workload mismatch: Did pain start after longer desk hours, driving, or stress?
That's why PT often finds causes that aren't obvious. The pain may be in the knee, but the problem may include hip weakness, ankle stiffness, or poor balance. The pain may be in the low back, but the driver may be repeated bending, bracing, fear of movement, or lack of trunk control.
For patients who want a better sense of how clinicians apply evidence instead of guesswork, this overview of integrating research in physical therapy is a useful read.
What happens during treatment
Treatment isn't a one-size-fits-all list of stretches. It's a plan built around your movement, symptoms, goals, and tolerance.
That plan usually includes a mix of the following:
| Focus | What the therapist is trying to change |
|---|---|
| Movement quality | Reduce patterns that keep irritating tissues |
| Strength and control | Build support around vulnerable joints |
| Mobility | Restore motion where stiffness is forcing compensation |
| Confidence | Help you move without guarding every step |
Pain management physical therapy is partly physical and partly educational. People improve faster when they understand why a movement hurts and what to do about it.
The bigger idea is simple. PT doesn't just treat soreness. It teaches your body, and often your nervous system, a safer and stronger way to function.
How Physical Therapy Calms Pain and Restores Movement
People sometimes think PT is just “a few exercises.” That misses how pain changes the body. When pain sticks around, tissues can get irritated, muscles can stop sharing work well, and the nervous system can become more protective than helpful. Physical therapy works because it addresses all three.
First, calm what's irritated
Some pain starts with tissue overload. A joint gets stiff. A tendon gets angry. Muscles guard an area because they're trying to protect it. In the early stage, the goal isn't to force intensity. It's to reduce irritation enough that normal movement becomes possible again.
That can mean hands-on treatment, better positioning, guided mobility work, or changing how you move through your day. We often tell patients that pain relief doesn't always start with doing more. Sometimes it starts with doing the right amount, in the right way.
Then rebuild support around the painful area
A painful shoulder, spine, knee, or hip often lacks a reliable support system. One muscle group overworks while another underperforms. The result is strain, compensation, and repeated flare-ups.
Strengthening and controlled loading matter. The goal isn't bodybuilding. The goal is giving your body a better scaffold so everyday tasks stop feeling like a threat.
A randomized controlled trial found that people with non-specific chronic low back pain who received physical therapy methods combined with exercise and medical treatment had better improvements in pain and functional status than those who received exercise and medical treatment without physical therapy, and those gains persisted for three months after treatment according to this PubMed Central study on chronic low back pain and physical therapy.
Finally, retrain the alarm system
Chronic pain isn't always a sign that damage is getting worse. Sometimes the nervous system becomes too sensitive. Movement that should feel safe starts feeling dangerous. People brace, avoid activity, and get caught in a cycle where less movement leads to more stiffness and more fear.
That's why graded movement works so well. You don't jump from avoiding stairs to doing everything at once. You build tolerance in steps. The body learns. The nervous system learns too.
A common example is desk-related neck or back pain. Many people need more than generic reminders to “sit up straight.” They need movement breaks, workstation changes, and targeted exercises. If that sounds familiar, this guide on how to fix your desk posture can complement what we teach in the clinic.
Why this matters for back and neck pain
Back and neck pain often respond best when treatment combines mobility, strength, and movement retraining instead of relying on one tool. We explain that in more depth in our guide on how physical therapy helps with back and neck pain.
Clinical reality: The exercise only works if it matches the problem. The same stretch that helps one person can aggravate someone else.
That's why good PT feels specific. Not random. Not generic. It follows the mechanics of your pain.
Your Personalized Toolkit of PT Techniques
When people hear “physical therapy,” they often picture a resistance band and a printed exercise sheet. That's part of it, but not the whole picture. Pain management physical therapy usually uses two categories of care: passive techniques and active techniques. Both have a role. They just don't do the same job.
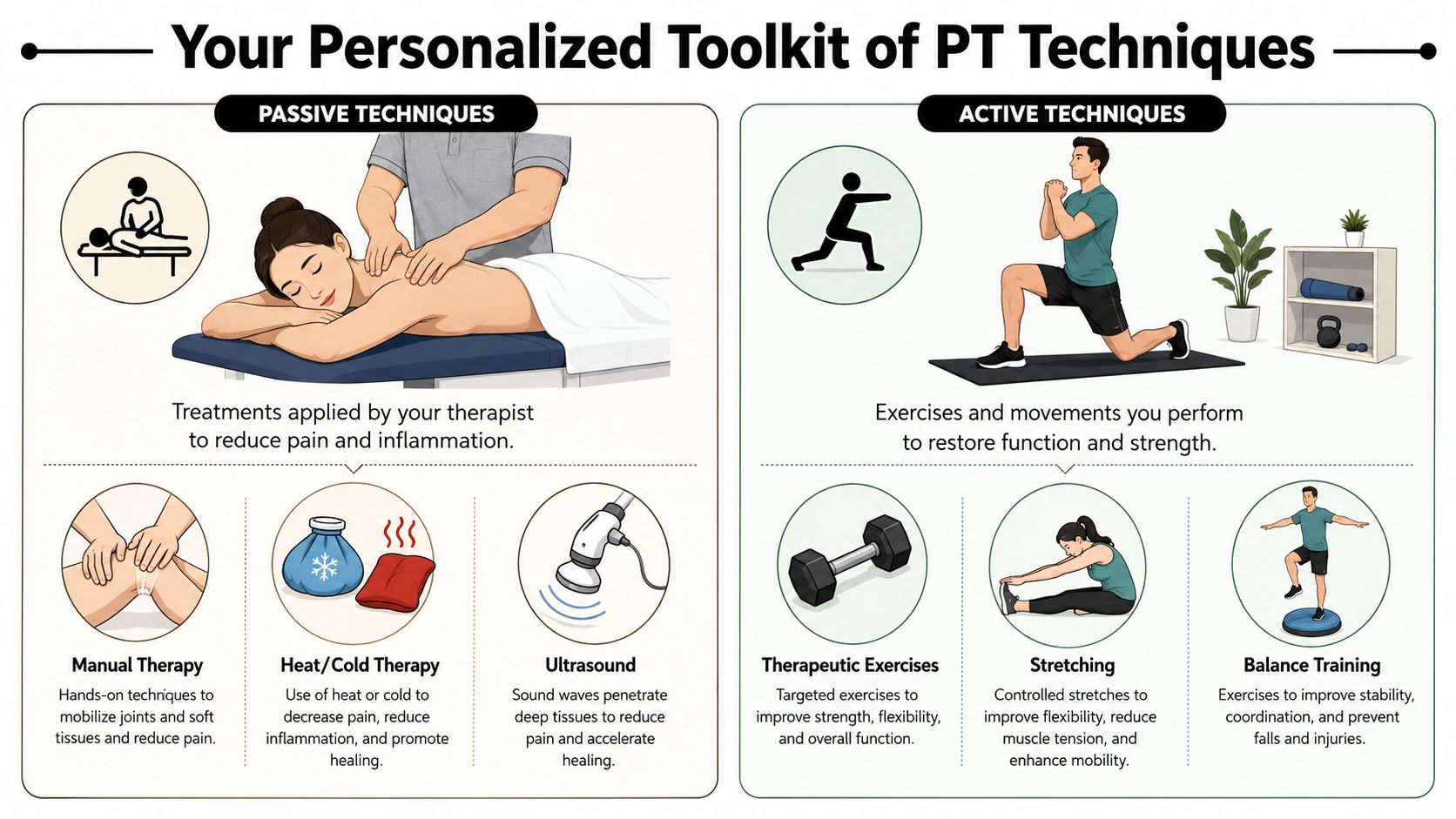
Passive tools help you get started
Passive treatments are things the therapist applies to you. These can be useful when pain is high, movement is guarded, or an area is too irritated to load well yet.
Common examples include:
- Manual therapy: Hands-on techniques to improve joint motion, reduce muscle tension, and help stiff areas move more normally.
- Heat or cold: Helpful for symptom relief and for making movement more tolerable in the short term.
- Electrical stimulation or ultrasound: Sometimes used selectively to calm symptoms or prepare an area for exercise.
Passive care can create an opening. It can reduce resistance, lower guarding, and help you move with less apprehension. But by itself, it usually doesn't build lasting resilience. That's why we don't want patients stuck in a cycle of “feel better for a day, then start over.”
For readers curious about hands-on options, our page on manual physical therapy techniques explains where manual treatment fits.
Active care creates lasting change
Active treatment is where long-term progress happens. This includes strengthening, stretching, balance work, walking programs, core control, and functional drills that match your life.
A guideline on physical therapy management for chronic pain reports that therapeutic exercise programs incorporating strengthening, stretching, aerobic conditioning, and functional activities show a statistically significant reduction in pain intensity and improvement in function, and that active exercise interventions reduce pain scores by an average of 1.8 points on a 10-point scale according to the MASAC guidance on physical therapy management for chronic pain.
That same source notes the strongest effects were seen in programs that combined exercise with other support. That matches what we see in practice. Exercise works best when the program is individualized, progressed properly, and paired with education.
What works and what doesn't
Here's the short version:
| Approach | What usually happens |
|---|---|
| Only passive treatment | Temporary relief, limited carryover |
| Random online exercises | Inconsistent results, possible flare-ups |
| Targeted active program | Better function, stronger tolerance, more confidence |
At clinics such as MedAmerica Rehab Center, the practical goal is to match the right combination of hands-on treatment, guided exercise, and progression to the person in front of us. That's what makes a plan feel personal instead of prewritten.
Treating Your Pain From Backache to Arthritis
Pain management physical therapy only makes sense if it applies to the problem you're living with. The treatment plan for sciatica shouldn't look like the plan for knee arthritis. A good program uses the same principles, but the details change based on the condition, the irritability of symptoms, and your goals.

Chronic low back pain and sciatica
Low back pain is one of the most common reasons people seek PT, and research described earlier supports its benefit in chronic cases. In practice, we often work on mobility where the spine or hips are stiff, then build trunk and hip strength so the back isn't doing all the work.
If sciatic symptoms are involved, the program may also include nerve-friendly movement, walking tolerance, posture changes, and gradual return to bending, lifting, or sitting. The key is not chasing pain with forceful stretching when the nerve is already irritated.
Knee arthritis and daily mobility
With knee arthritis, we usually think in layers. First, make walking, standing, and stair use less aggravating. Then improve strength in the muscles that help absorb load, especially around the hips and thighs. Better control above and below the knee often reduces stress at the joint itself.
Our page on physical therapy for arthritis gives a closer look at how these plans are structured. Some patients also like reading broader self-care resources, such as this NexiHerb joint care guide, to understand common support strategies outside the clinic.
Neck pain, headaches, and posture strain
Neck pain often involves more than the neck. We may find limited upper-back motion, weak shoulder blade support, jaw tension, or work habits that keep the head forward for hours at a time.
In those cases, treatment often combines mobility work, postural retraining, and exercises that make holding your head up feel less effortful. Patients are often surprised that better shoulder and thoracic control can reduce what they thought was “just neck pain.”
Post-surgical or post-injury recovery
After surgery or injury, pain isn't the only issue. There may also be swelling, stiffness, weakness, and a loss of confidence in the affected area. PT helps restore motion first, then control, then endurance for real life tasks.
If a program doesn't match the stage of healing, it won't feel right. Too much too soon can flare things up. Too little for too long slows recovery.
The right pace matters as much as the right exercise.
Your Role in Achieving Lasting Pain Relief
This is the part many clinics don't explain clearly enough. Your recovery doesn't depend only on what happens during appointments. It depends on what happens between them.
That doesn't mean you need to spend your life exercising. It means the body changes through repetition. One good session can help. Consistent follow-through is what makes the improvement stick.
What patients do that helps most
The people who make steady progress usually do a few things well:
- They practice the home plan regularly: Not perfectly, just consistently.
- They report flare-ups openly: That helps us adjust the program instead of guessing.
- They measure success by function: Walking farther, sleeping better, lifting easier, getting through the day with less guarding.
- They stay engaged even when pain doesn't vanish immediately: Progress is often uneven before it becomes stable.
That last point matters most in chronic pain.
A realistic view of chronic pain care is that PT often aims to improve function, flexibility, strength, and daily activity tolerance, not guarantee complete pain elimination. For some conditions, especially long-term pain, nerve-related pain, or complex pain patterns, the most effective approach is often a combined plan that matches treatment to the pain mechanism and sets realistic goals, as described in this discussion of the role of physical therapy in pain management.
What success may look like
Success may mean:
- getting out of bed without bracing yourself first
- walking the dog without paying for it later
- carrying groceries with more confidence
- sleeping through the night more often
- playing with grandkids, gardening, or driving with less fear
Those wins count even if some pain remains.
What we tell patients: Don't wait to feel perfect before you start living again. Build capacity, then let life expand around it.
What usually doesn't work
People tend to stall when they bounce between total rest and overdoing it, when they stop moving out of fear, or when they expect one technique to solve everything. Chronic pain rarely responds well to all-or-nothing behavior.
The more effective path is steady, guided progression. That's less dramatic, but much more reliable.
Starting Your Recovery Journey in Deerfield Beach
Starting physical therapy shouldn't feel complicated. Patients often just want to know three things. Can I get in soon, will my insurance be handled clearly, and what happens at the first visit?
At our Deerfield Beach clinic, the process is meant to be straightforward and low-stress.
What happens first
When you call or reach out online, the front desk helps with scheduling, basic intake, and insurance questions. If you've had imaging, a referral, surgery, or a recent injury, it helps to mention that early so the team can prepare for your visit.
Same-day availability may be possible depending on the schedule. If you're dealing with an auto accident injury, workers' compensation issue, or post-surgical pain, say that upfront so the paperwork path is clear from the beginning.
What to expect at the first appointment
The initial evaluation is where the important work begins. Expect a detailed conversation about your symptoms, what aggravates them, what eases them, and what you want to get back to doing. That part matters as much as the physical exam.
Then your therapist looks at movement, strength, flexibility, balance, and functional tasks that relate to your pain. You may walk, bend, reach, stand from a chair, or perform simple tests that help identify what is driving symptoms.
A strong first visit usually ends with three things:
- A working explanation of why you're hurting and what patterns need to change.
- A treatment plan with clear priorities, not a vague promise to “see how it goes.”
- A first set of actions you can start right away at home.
Why people feel more confident after the evaluation
Uncertainty makes pain harder to live with. Once people understand what's going on, what the trade-offs are, and what progress should look like, they usually feel more in control.
That's the true beginning of recovery. Not when pain disappears overnight, but when the path forward stops feeling mysterious.
If pain has been shrinking your world, MedAmerica Rehab Center can help you take the next practical step. Reach out to schedule an evaluation in Deerfield Beach, get clear answers about what's driving your symptoms, and start a plan focused on moving better, functioning better, and getting back to the parts of life you miss.