Your Guide to Degenerative Disc Disease Treatment Cervical
You wake up, turn your head toward the alarm, and feel that familiar catch in your neck again. By mid-morning, checking your blind spot while driving is annoying, looking down at your phone feels worse, and you're starting to wonder whether this is just a stubborn muscle knot or something deeper.
That concern is reasonable. Persistent neck pain can wear you down because it doesn't stay in one part of life. It shows up at your desk, in the car, during sleep, and sometimes all the way into your shoulder or arm. When someone is told they have cervical degenerative disc disease, the name alone can sound more alarming than the condition itself.
In plain language, this diagnosis usually means the discs in your neck have changed over time. That's common, and in many cases it's manageable. The bigger question isn't just what the MRI says. The bigger question is whether your symptoms point to a straightforward mechanical neck problem or whether a nerve or even the spinal cord is being affected.
If you've been searching for answers, it helps to start with a grounded picture of symptoms of degenerative discs in the neck. From there, the right treatment plan becomes much clearer.
That Nagging Neck Pain Might Be More Than a Kink
A lot of people dismiss early neck symptoms because they come and go. Maybe it started after a long week at a computer. Maybe after a poor night's sleep. Maybe after years of looking down at a phone, lifting at work, or carrying tension in the shoulders.
Then the pattern changes.
The stiffness lasts longer. You stop rotating your head fully. You start moving your whole body to look sideways. Some days the pain feels local and achy. Other days it spreads toward the shoulder blade. That's often when people start asking whether they need imaging, injections, or surgery.
Why the name sounds worse than it is
Cervical degenerative disc disease doesn't automatically mean a dangerous spine problem. It usually refers to age-related or wear-related changes in the discs of the neck. Those discs act like spacers and shock absorbers between the bones of the cervical spine. Over time, they can lose some of their normal height and flexibility.
That can create pain, stiffness, and sensitivity to certain positions. It can also change how the nearby joints and muscles work. But many people with these changes improve with the right conservative care.
Practical rule: A painful neck doesn't always mean a serious neck problem. The details that matter most are where the pain goes, whether weakness is developing, and whether coordination or balance is changing.
What patients usually want to know first
Individuals aren't asking for anatomy lessons. They want clear answers to practical questions:
- Can this be treated without surgery?
- Is the pain coming from the disc itself, a pinched nerve, or something more serious?
- What should I stop doing right now?
- How long should I try conservative care before worrying?
Those are the right questions. A useful approach to degenerative disc disease treatment cervical cases starts with symptom pattern, movement testing, and neurologic screening, not fear.
What Is Happening Inside Your Neck
Think of the discs in your neck like shock absorbers. They help each spinal segment move smoothly and keep space available for nearby nerves. When a disc degenerates, it usually loses some hydration and resilience. It may flatten, stiffen, or irritate surrounding structures.
That doesn't mean the disc is “gone” or that your neck is crumbling. It means the tissue has changed, and your body may react with pain, muscle guarding, and reduced motion.

The mechanics behind the pain
A healthier disc usually distributes load well. A degenerated disc may tolerate certain positions poorly, especially prolonged looking down, sustained sitting, repeated extension, or abrupt rotation. The surrounding joints can stiffen. Muscles in the neck and upper back often tighten to protect the area, which can create its own cycle of pain.
Common contributors include:
- Natural aging changes that affect disc hydration and elasticity
- Past strain or injury that changed how a segment moves
- Postural loading from long periods of desk work or device use
- Genetic tendency that influences how quickly disc tissue changes
Some patients feel mostly local neck pain. Others notice pain into the upper trapezius or around the shoulder blade. Symptoms can be mechanical, meaning they worsen with certain positions and improve when load is reduced.
Local pain versus nerve symptoms
This distinction matters more than is commonly understood.
A mechanical neck pain pattern often includes stiffness, soreness, painful turning, and discomfort after prolonged posture. The pain may stay in the neck or upper shoulder region.
A nerve-related pattern can look different:
- Pain traveling down the arm
- Tingling or numbness in the hand or fingers
- Grip weakness or trouble lifting the arm
- Burning, shooting, or electric-type pain
Those symptoms raise concern for radiculopathy, which means a nerve root may be irritated or compressed. A more urgent category is myelopathy, where the spinal cord itself is affected. That can produce clumsiness, hand coordination problems, gait changes, or balance difficulty.
For patients trying to make sense of reports and terminology, even administrative topics like fixing cervical myelopathy coding denials can highlight how important it is to distinguish routine degenerative findings from true spinal cord involvement.
Neck imaging labels can sound dramatic. Symptoms and neurologic findings tell you whether those labels are clinically important.
Why one MRI word can mislead you
Many people see “degeneration,” “bulge,” or “spondylosis” on a report and assume surgery is inevitable. It isn't. Imaging findings only become meaningful when they match your symptoms and exam.
That's why a good exam doesn't stop at the scan. It asks a better question. Is this a painful but manageable neck condition, or is the nervous system being affected in a way that changes the treatment plan?
Getting an Accurate Diagnosis for Your Neck Pain
A strong diagnosis starts with a conversation, not a scanner. The history often reveals more than people expect. When did the pain start? Is it constant or position-dependent? Does it stay in the neck, travel into the arm, or affect hand function? Are there headaches, dropping objects, or trouble with fine motor tasks?
Those details help separate a typical cervical degenerative pattern from radiculopathy or myelopathy.
What a physical exam is looking for
During an exam, a clinician usually checks how your neck moves, which motions reproduce symptoms, how your shoulder and upper back move, and whether certain positions centralize or spread pain. Muscle testing matters too. If one side is weaker, that may point to nerve involvement rather than simple guarding.
Reflexes, sensation, and coordination are just as important. A person with local neck stiffness and pain on rotation may stay on a conservative path. A person with progressive weakness, altered reflexes, hand clumsiness, or balance change needs a different level of attention.
A practical overview of when you need an MRI and when you need an X-ray can help patients understand why imaging is sometimes useful and sometimes overused.
What imaging can and cannot tell you
An X-ray can show alignment and degenerative changes. An MRI can show discs, nerves, and the spinal cord in more detail. Those tools are helpful when the exam suggests nerve compression, when symptoms aren't improving as expected, or when surgery is being considered.
But imaging doesn't replace clinical reasoning.
| What imaging helps with | What imaging cannot do alone |
|---|---|
| Show disc changes and narrowing | Prove which finding is causing pain |
| Reveal possible nerve or cord compression | Measure how much a symptom matters functionally |
| Support surgical planning | Replace a strength, reflex, and coordination exam |
The diagnosis patients actually need
The most useful diagnosis is not just “you have degeneration.” It's something more specific:
- Mechanical neck pain likely related to disc and joint changes
- Neck pain with arm symptoms suggesting nerve root irritation
- Signs that raise concern for spinal cord involvement
That distinction drives treatment. It also helps patients avoid two common mistakes: ignoring nerve warning signs, or panicking over an MRI report that may not match their symptoms.
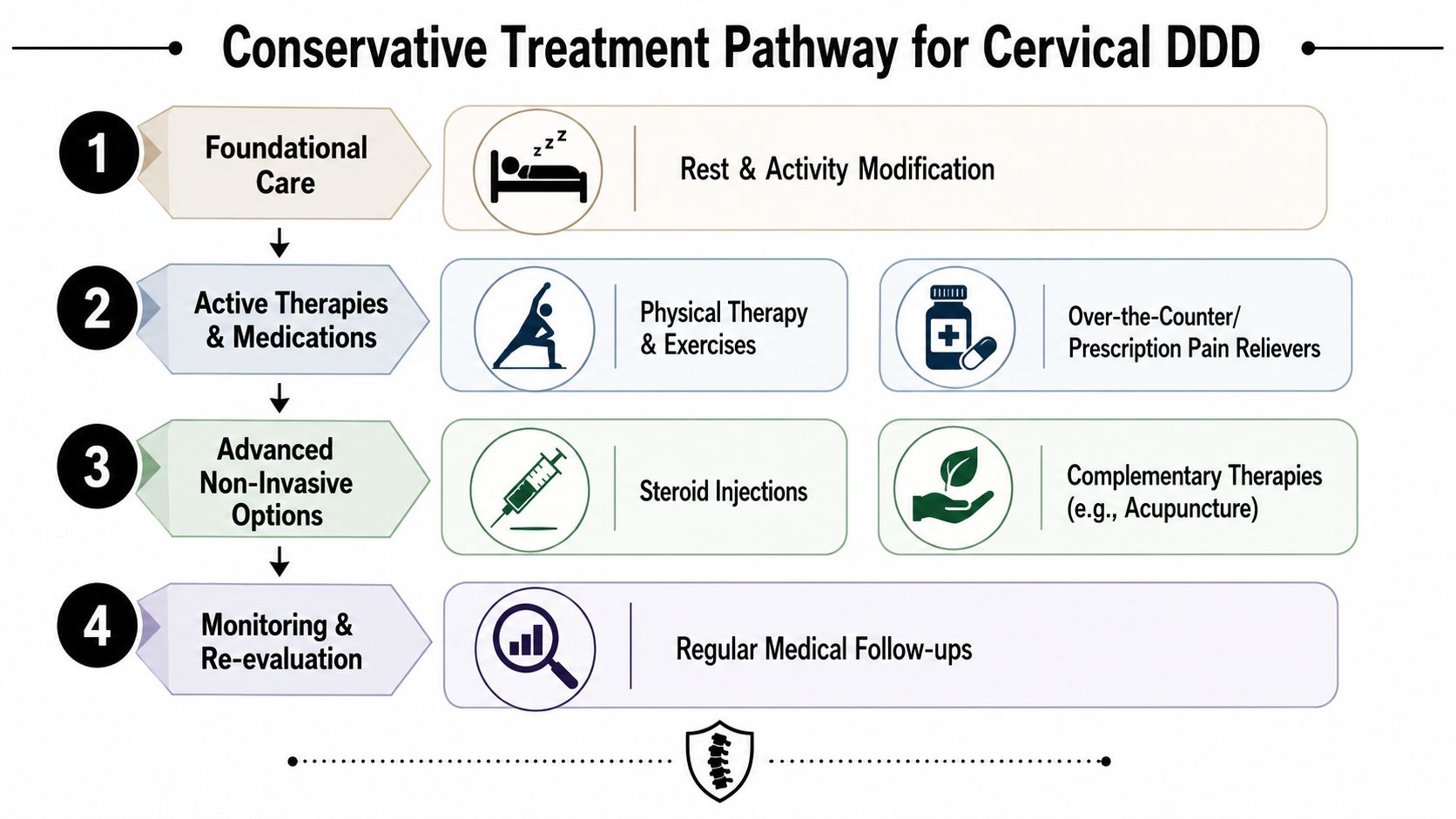
Your First Line of Defense Conservative Treatments
For many individuals, the best starting point is not surgery. It's a structured conservative plan aimed at reducing pain, restoring motion, improving muscle support, and preventing repeat flare-ups. Major clinical guidance describes cervical degenerative disc disease as usually managed nonoperatively first, with care centered on pain relief, function, and recurrence prevention. It also notes excellent or good outcomes in 70% to 90% of cases overall, and reports that targeted exercise-based programs often produce measurable improvements in pain and disability within 4 to 12 weeks according to clinical guidance on cervical disc degeneration management.
That matters because conservative care isn't the same as doing nothing. It's active treatment.
What tends to work best first
Physical therapy is often the backbone of treatment because it addresses the problem from multiple angles at once. A good program doesn't just stretch your neck. It looks at cervical mobility, deep neck flexor control, scapular strength, thoracic mobility, posture tolerance, and the movements that trigger your symptoms.
Hands-on care can also help when the neck is guarded and movement is limited. Soft tissue work, joint mobilization, and guided movement retraining often make exercise more tolerable. The point isn't to chase temporary relief only. The point is to make lasting movement improvement possible.
Supportive treatments may include:
- Medication support such as short-term anti-inflammatory or pain-relieving medication when appropriate, guided by your physician
- Activity modification so you reduce aggravating loads without complete rest
- Heat or ice depending on whether stiffness or irritation is the bigger issue
- Sleep and workstation changes to reduce repeated strain on the neck
For people who want a practical overview, this guide on how physical therapy helps with back and neck pain explains why movement-based care is often the center of a good plan.
Treatments that can help, and their trade-offs
Not every conservative option fits every patient. The right choice depends on symptom pattern.
| Treatment | Best use | Trade-off |
|---|---|---|
| Physical therapy | Restoring motion, strength, and movement confidence | Requires consistency and progression |
| Manual therapy | Reducing guarding and improving mobility | Relief may be short-lived if not paired with exercise |
| Chiropractic care | Some patients respond well for mobility-related symptoms | Needs careful patient selection, especially if nerve signs are present |
| Acupuncture | Can help calm pain sensitivity and muscle tension | Usually works best as part of a broader plan |
| Injections | May reduce pain enough to participate in rehab | Doesn't rebuild strength or fix poor movement habits |
| Short-term medication | Useful during painful flare periods | Not a long-term correction strategy |
What often doesn't work well on its own
Patients lose time when treatment becomes too passive for too long. Common examples include repeated massage without exercise progression, prolonged use of a soft collar, complete activity avoidance, or random internet stretches that don't match the symptom pattern.
A neck with degenerative changes usually needs two things at once: symptom control and gradual reloading.
Clinical reality: If treatment reduces pain for a day but your neck still can't tolerate sitting, turning, lifting, or driving, the plan isn't finished.
A sample conservative pathway
This video gives a visual sense of how movement-based care can fit into recovery.
A practical course of care often looks like this:
Calm the flare first
Reduce the most provocative positions, improve sleep setup, and use symptom-relieving techniques so pain isn't constantly escalating.Restore movement next
Work on cervical rotation, extension tolerance if appropriate, thoracic mobility, and shoulder blade mechanics.Build support around the neck
Strengthen the deep neck flexors, scapular stabilizers, and upper back so the neck isn't doing all the work alone.Return to real-life tasks
Practice driving rotation, desk posture breaks, lifting form, and exercise tolerance so progress transfers into daily life.
In a multidisciplinary setting, one option patients may encounter is MedAmerica Rehab Center, where physical therapy, chiropractic care, acupuncture, and shockwave therapy are available as part of individualized non-surgical management. The important point is not the label of the clinic. It's whether the plan is specific, progressive, and responsive to your symptoms.
When conservative care is going well
You don't need pain to disappear overnight to know treatment is helping. Meaningful progress often looks like:
- Less morning stiffness
- Improved head turning while driving
- Fewer arm symptoms
- Longer sitting tolerance
- Less fear around normal movement
That's the goal of degenerative disc disease treatment cervical cases at the conservative stage. Not just a lower pain score, but a better-functioning neck.
When Surgery Becomes the Right Option
Surgery should be considered calmly, not as a reflex to an MRI finding. The central question is whether symptoms suggest a more serious neurologic problem or whether a patient has failed a solid course of conservative care.
Academic guidance emphasizes that the decision to escalate often depends less on the image itself and more on persistent radicular pain, progressive muscle weakness, or signs of spinal cord compression that do not respond to conservative care, as described in guidance on cervical radiculopathy and myelopathy.
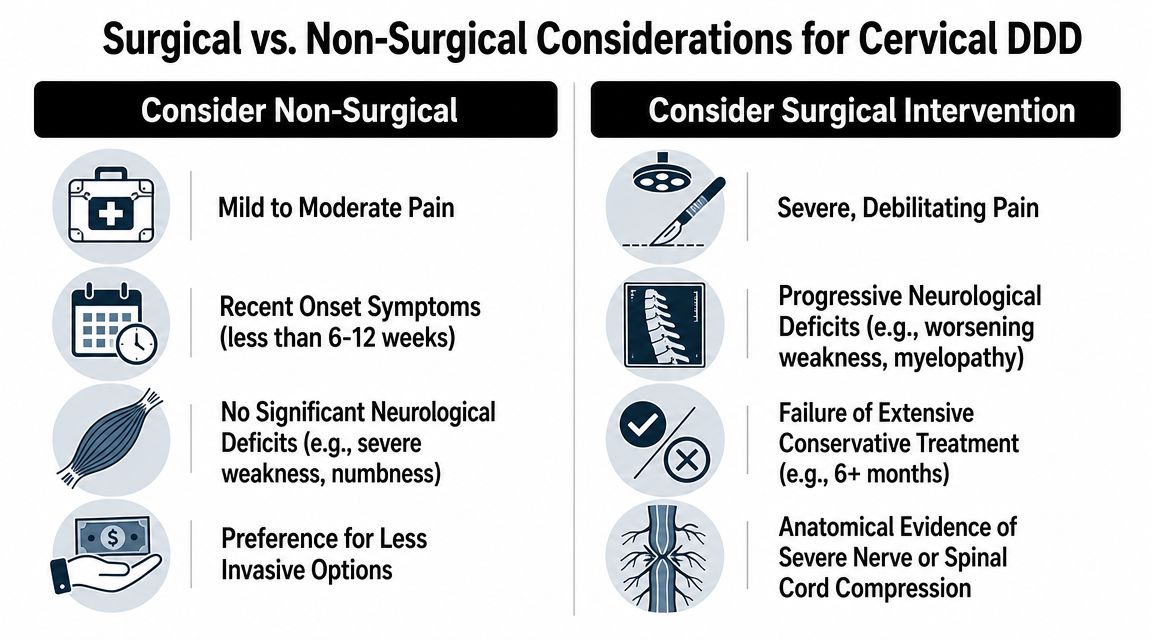
Signs that should change the conversation
Typical mechanical neck pain can be frustrating, but it usually stays in the realm of conservative treatment. Surgery enters the picture when the pattern changes.
Red flags for surgical evaluation often include:
- Arm pain that persists despite appropriate conservative care
- Worsening weakness in the shoulder, arm, or hand
- Loss of dexterity, such as trouble buttoning clothes or handling small objects
- Balance difficulty or gait change
- Neurologic dysfunction that suggests spinal cord involvement
A patient with pain and stiffness alone is different from a patient whose hand is getting weaker or less coordinated. That distinction matters more than dramatic wording on an imaging report.
Non-surgical versus surgical thinking
| Consider continued non-surgical care | Consider surgical consultation |
|---|---|
| Neck pain is mainly local or posture-related | Symptoms are clearly neurologic and progressive |
| Function is limited but improving with rehab | Weakness is worsening or not recovering |
| Symptoms fluctuate but don't steadily deteriorate | Signs suggest spinal cord compression |
| Movement-based treatment is still producing gains | Conservative care has not changed the clinical course |
If you're getting stronger, moving better, and your symptoms are trending in the right direction, surgery is usually not the next step.
The common procedures patients hear about
When surgery is appropriate, patients often hear about ACDF and artificial disc replacement.
ACDF stands for anterior cervical discectomy and fusion. In simple terms, the surgeon approaches the spine from the front of the neck, removes the problematic disc, relieves pressure on the nerve or spinal cord, and stabilizes the segment.
Artificial disc replacement also removes the damaged disc from the front, but instead of fusing the level, it places a device designed to preserve motion at that segment. Not every patient is a candidate. Selection depends on anatomy, the affected level, the rest of the spine, and the surgeon's judgment.
The goal of both is similar: decompress the involved neural structure and improve function. The trade-off is different. Fusion stabilizes but eliminates motion at that level. Disc replacement may preserve motion in selected cases.
When to seek faster evaluation
Call promptly if you notice progressive weakness, increasing clumsiness, or changes in walking and balance. Those symptoms deserve attention sooner rather than later. In those cases, the issue may not be degenerative disc pain alone. It may be nerve root or spinal cord compromise, and that changes everything.
The Road to Recovery and Long-Term Wellness
Recovery isn't one event. It's a process of reducing irritability, rebuilding capacity, and keeping the neck from sliding back into the same overload pattern.
That process looks different depending on whether you recover with conservative treatment or after surgery, but both paths require active participation.
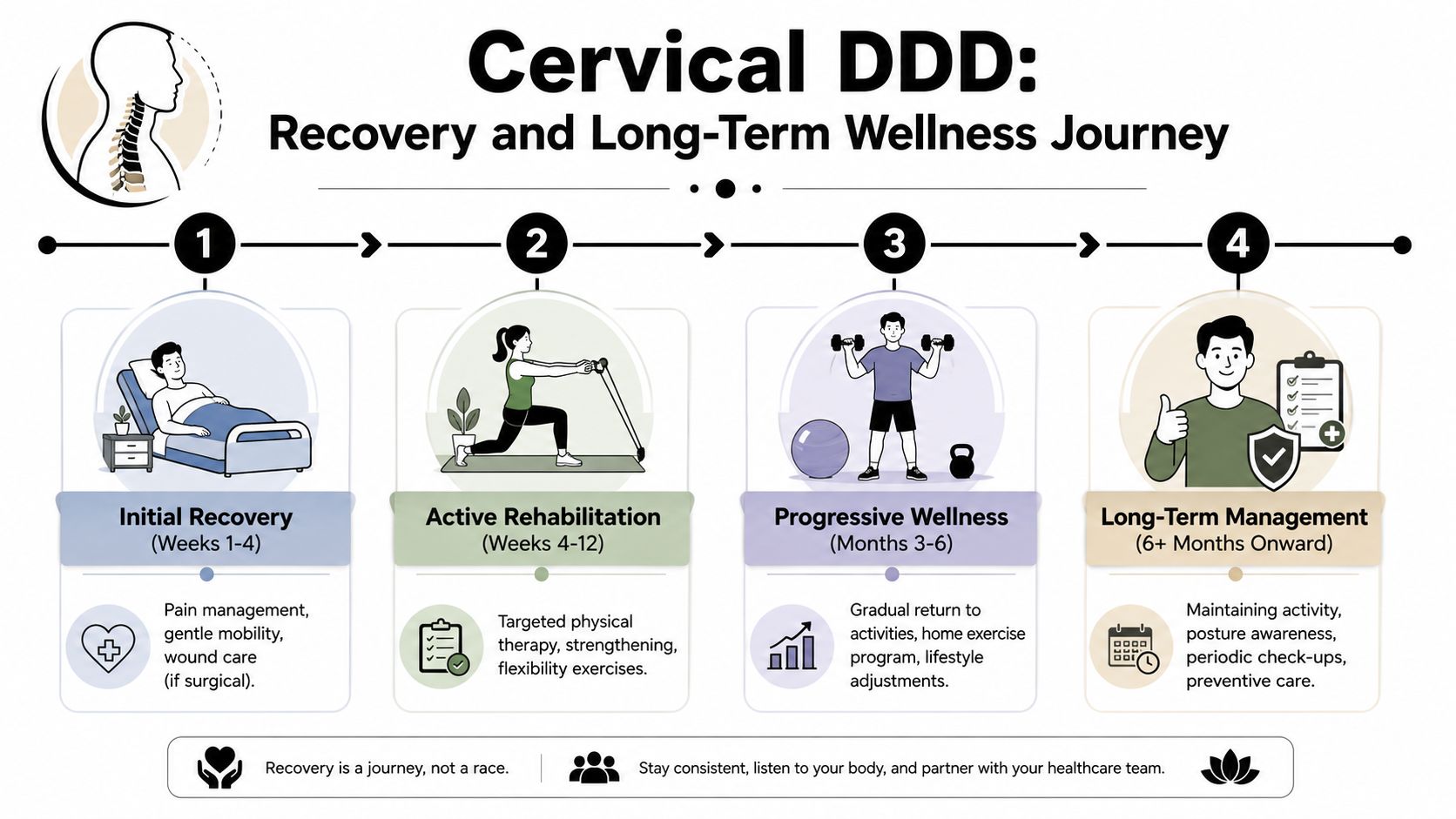
If you improve without surgery
Most non-surgical recoveries move through recognizable phases. Early on, the focus is calming symptoms and restoring enough motion for daily tasks. After that, the work shifts toward endurance, posture tolerance, and strength around the neck and shoulder girdle.
What keeps results from fading is usually simple, not fancy:
- A home exercise routine you'll consistently follow
- Better desk and driving setup
- Regular movement breaks
- Less time in sustained forward-head posture
- Confidence returning to normal activity
The best long-term plans are realistic. If a program only works in the clinic and never fits your life, it won't last.
If you have surgery
Post-surgical recovery still includes rehabilitation. Early goals usually involve protecting healing tissues, restoring safe mobility, and gradually returning to daily activity. Later phases focus on rebuilding neck and upper-quarter strength, improving posture, and preventing compensation patterns.
Patients sometimes assume surgery eliminates the need for therapy. Usually it changes the rehab plan rather than removing it. You still need your shoulders, upper back, and neck muscles to work well together.
Recovery goes better when patients stop asking, “How fast can I get back?” and start asking, “What capacity do I need to build so this holds up?”
What long-term neck health looks like
Long-term success is less about perfection and more about management. Flare-ups can still happen. The difference is that you understand what they mean and what to do next.
A durable plan usually includes:
- Maintenance mobility for the neck and thoracic spine
- Strength work for the deep neck flexors and scapular stabilizers
- Load awareness during work, lifting, and exercise
- Prompt reassessment if symptoms shift into numbness, weakness, or balance change
That's how a short-term fix becomes long-term wellness.
How MedAmerica Rehab Center Can Help You
Neck pain becomes less intimidating when the plan is clear. Start by identifying whether your symptoms look mechanical, nerve-related, or more urgent. Then match treatment to that pattern instead of chasing random remedies.
At MedAmerica, care is built around conservative, function-focused treatment first. That includes physical therapy, chiropractic care, acupuncture, and individualized rehab plans aimed at reducing pain, improving movement, and helping patients avoid unnecessary surgery or medication. For someone with cervical degenerative symptoms, that kind of coordinated approach is often what turns scattered symptom management into a real recovery plan.
Good support also matters between visits. For practices looking at ways to improve communication and responsiveness, tools like LeadBlaze's patient care chatbot show how healthcare teams can answer common questions and help patients stay engaged with care.
If you're in Deerfield Beach or a nearby community and your neck pain isn't settling down, getting examined early can save a lot of frustration. The right exam can tell you whether you're dealing with manageable cervical DDD, a nerve issue that needs closer monitoring, or a problem that should be escalated sooner.
If your neck pain is limiting work, sleep, driving, or daily movement, schedule an evaluation with MedAmerica Rehab Center. A focused exam can identify whether your symptoms fit a conservative rehab plan or need further medical evaluation, so you can start the right treatment with confidence.