Carpal Tunnel Treatment Options: Your Complete Guide
You wake up in the middle of the night with your hand buzzing. You shake it out, flex your fingers, wait for the pins and needles to settle down, and try to get back to sleep. The next morning, you grab a coffee mug and almost drop it. Later, buttoning a shirt or holding a phone feels strangely awkward.
That pattern is familiar to a lot of people with carpal tunnel syndrome. It often starts as an annoyance. Then it begins to interrupt sleep, work, exercise, driving, and basic hand use. The good news is that you usually have more than one path forward.
Some carpal tunnel treatment options are simple and practical. Some are more targeted and clinical. Some help symptoms but don't change the pressure on the nerve. Others address the mechanical problem more directly. Knowing the difference matters, because it helps you stop wasting time on treatments that only cover up pain.
That Tingling Feeling Is Not Your Imagination
For many people, carpal tunnel doesn't begin with a dramatic injury. It creeps in. Nighttime numbness. Tingling in the thumb, index finger, and middle finger. A hand that feels clumsy when you reach for keys, a toothbrush, or a steering wheel.
During the day, symptoms can be inconsistent enough to make you second-guess yourself. You may notice that typing, texting, gripping a book, or holding a hair dryer sets things off. Then the feeling eases, and you wonder if it's really a problem. It is.
When the median nerve is irritated at the wrist, symptoms can come and go before they become more persistent. That's one reason people wait too long to deal with it. They adapt. They shake the hand out. They switch hands. They push through.
Carpal tunnel symptoms are often most obvious at night, but the real issue is usually present all day.
The most useful way to think about treatment is not, "What can I take for this?" It's, "What's creating pressure on the nerve, and how do I reduce it?" That shift changes the whole conversation. Instead of chasing temporary relief, you start choosing care based on what improves hand function and protects the nerve over time.
What Is Carpal Tunnel Syndrome Anyway
Carpal tunnel syndrome happens when the median nerve gets compressed as it passes through a narrow space in the wrist called the carpal tunnel. That tunnel also contains flexor tendons, so it doesn't take much crowding or irritation for pressure to build.
A simple analogy helps. Think of the median nerve like a garden hose. If the hose gets pinched, flow drops. In the wrist, the "flow" is nerve signaling. When the nerve is compressed, the result can be numbness, tingling, pain, weakness, or loss of dexterity.
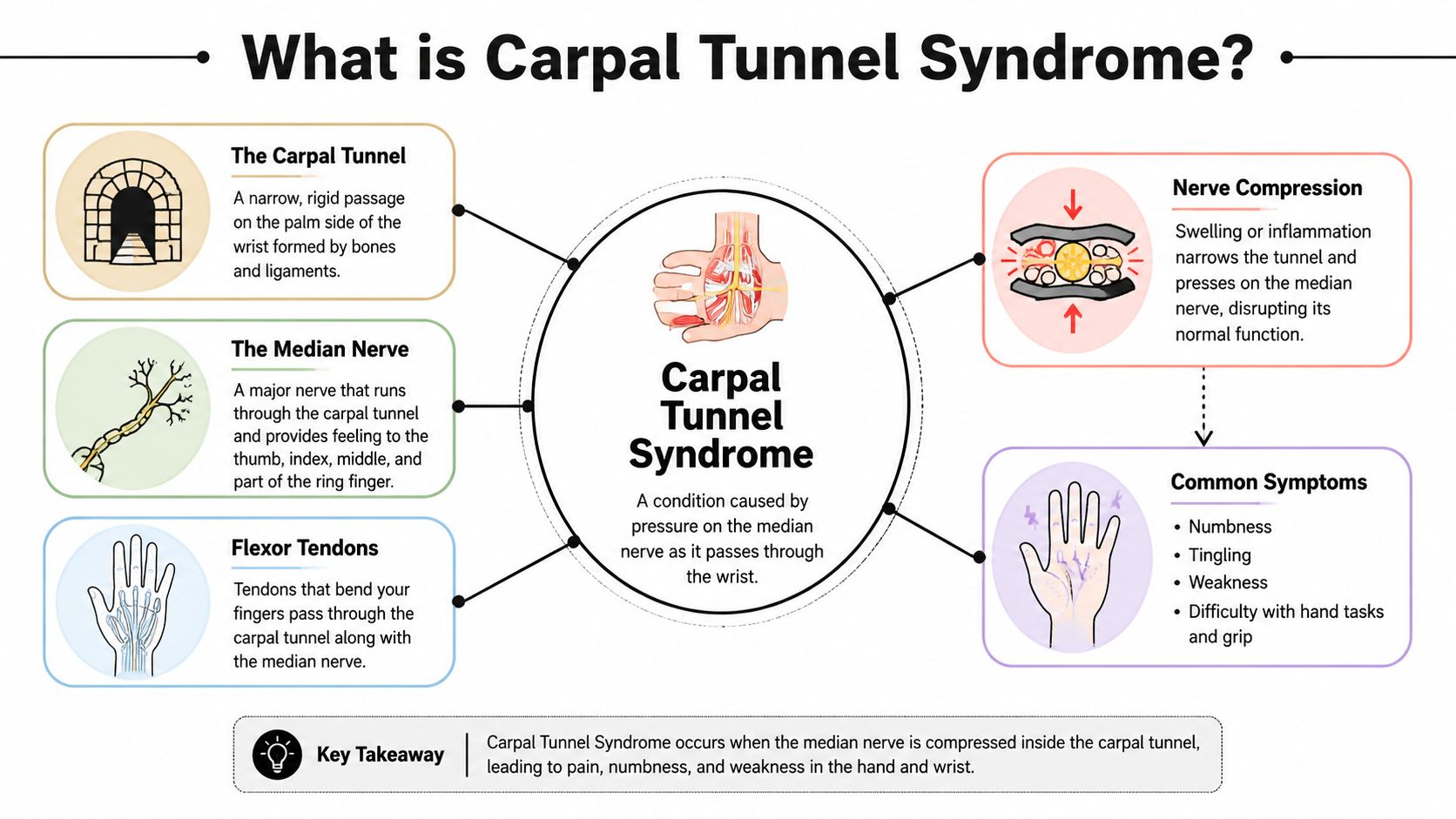
What the median nerve does
The median nerve helps provide feeling to the thumb and the next fingers on the palm side of the hand. It also supports some of the muscles involved in thumb movement. That's why carpal tunnel can affect both sensation and grip.
Common symptoms include:
- Numbness and tingling: Often felt in the thumb, index, middle, and part of the ring finger.
- Night symptoms: Many people wake up with a hand that feels asleep.
- Weakness: Grip can feel unreliable, especially with small objects.
- Pain or ache: Sometimes centered at the wrist, sometimes traveling into the forearm.
Why it happens
Carpal tunnel is a mechanical compression problem. The tunnel may become crowded because of tendon irritation, tissue swelling, wrist position, repetitive loading, anatomy, or health conditions that make nerves more vulnerable. Pregnancy, arthritis, and diabetes can also be part of the picture.
What matters for treatment is this: if pressure on the nerve is the problem, the best interventions are the ones that reduce that pressure, improve wrist mechanics, or create more space for the nerve to move without irritation.
That idea explains why some treatments help only briefly, while others have a better chance of producing lasting relief.
Your First Line of Defense Conservative Treatments
You wake up at 2 a.m. with a hand that feels asleep, shake it out, and get a few minutes of relief. The next day you buy a wrist brace and a bottle of ibuprofen. That is a common starting point, but it rarely works well if the positions and tasks irritating the nerve stay the same.
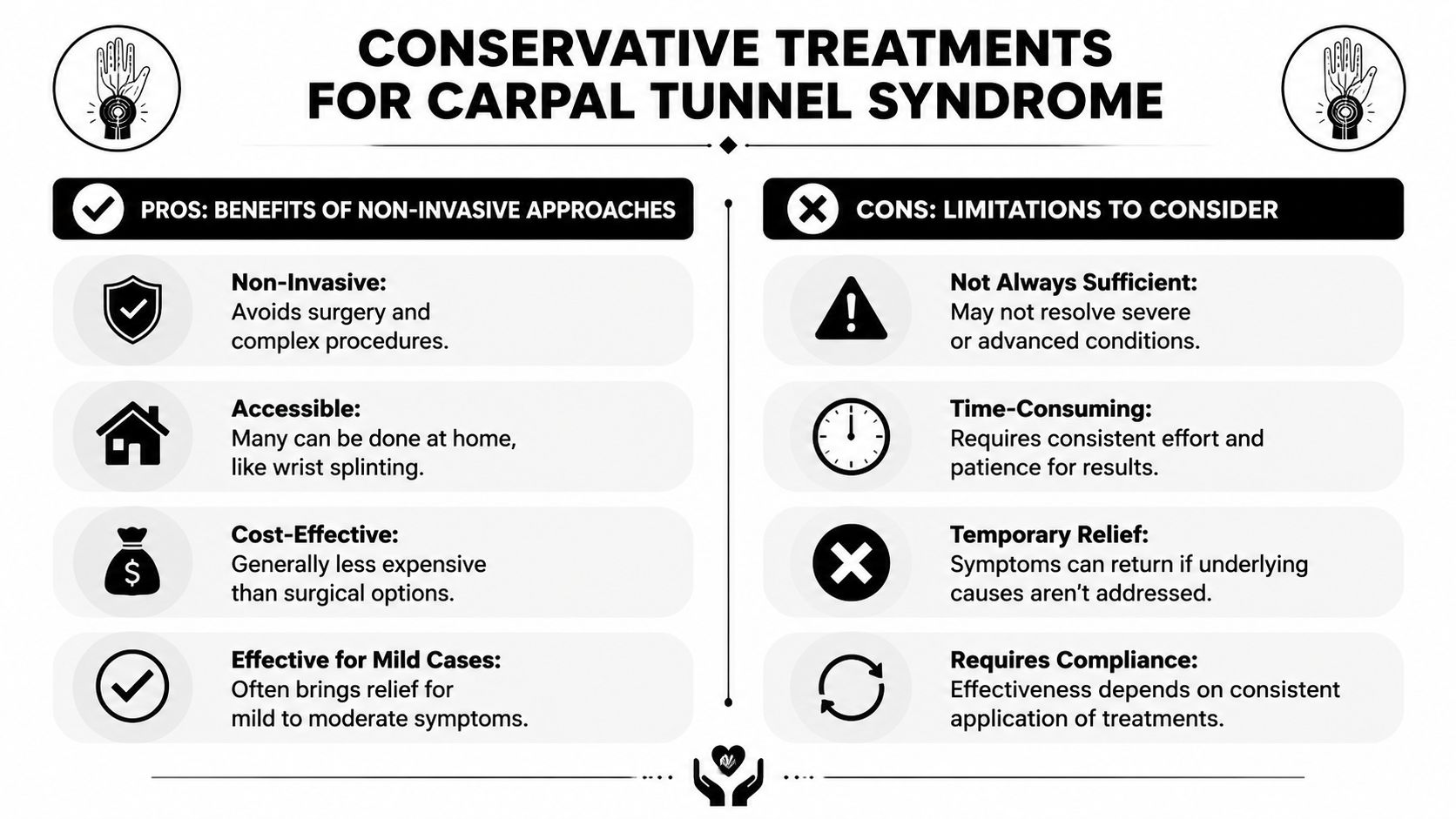
Night splints can help, but they have limits
For mild to moderate carpal tunnel symptoms, a night splint is often a reasonable first step. Its job is straightforward. It keeps the wrist closer to neutral during sleep, which can reduce overnight irritation of the median nerve.
That can make a real difference if numbness and tingling wake you up. It is one of the more useful passive tools because it targets a specific aggravating position.
Still, a splint only works during the hours you wear it. It does not change how you type, hold your phone, grip tools, lift bags, or sleep with your wrist curled under you. In clinic, I often see people who say the brace "helps some," but their daytime habits keep recreating the same stress that caused the flare in the first place.
Why NSAIDs often fall short
Ibuprofen or naproxen may take the edge off pain for a short time. That can be reasonable during a flare, especially when soreness is making it hard to rest.
The trade-off is simple. Pain relief is not the same as pressure relief. If the nerve is still being compressed by wrist position, repetitive gripping, or tissue crowding in the tunnel, medication does not solve the mechanical problem.
That is why long-term NSAID use tends to disappoint in carpal tunnel cases. Symptoms may calm down briefly, then return as soon as the same loading pattern comes back. If you need pain medication over and over just to get through normal tasks, it is time to change the plan.
Practical rule: Choose treatments that reduce irritation at the source, not just treatments that make symptoms easier to ignore.
Activity changes usually matter more than patients expect
The most effective early treatment is often less dramatic than people want. It is changing the hand and wrist positions that repeatedly provoke symptoms.
Conservative care either works or stalls. A brace can support you at night. Better mechanics during the day often determine whether the nerve settles down.
Focus on the tasks that bring on tingling, aching, or hand fatigue:
- Keyboard use: Keep the wrist straight and avoid resting it on a hard desk edge.
- Phone use: Reduce prolonged gripping and avoid scrolling with the wrist bent.
- Reading or tablet use: Bring the screen up instead of dropping the wrist into flexion.
- Sleeping posture: Keep the hand out from under the pillow or torso.
- Work demands: Break up repetitive pinching, forceful gripping, and sustained tool use when possible.
These sound like small adjustments. Repeated hundreds of times a day, they are not small at all.
If symptoms are tied to work or home routines, guided rehab can speed up the trial-and-error process. A therapist can identify the exact movements driving your symptoms and build a plan that includes task changes, mobility work, and graded exercise. For people who want that kind of support, hand physical therapy services can be one structured option.
A short home exercise video can also help you visualize safe movement strategies before your first appointment.
Professional Non-Surgical Interventions
When symptoms keep interfering with sleep, work, or grip despite home changes, it's time to consider more targeted non-surgical care. This stage isn't about doing more random things. It's about choosing treatments that match the mechanism of the problem.

Physical therapy and guided hand rehab
A good rehab program for carpal tunnel usually focuses on several questions at once. Is the wrist staying in irritated positions all day? Is the nerve moving poorly relative to surrounding tissue? Are the forearm and hand overloaded? Is there weakness or stiffness that keeps forcing compensation?
Treatment may include:
- Nerve gliding exercises: These aim to improve how the median nerve moves through surrounding tissue.
- Tendon gliding: Useful when stiffness and tendon crowding are part of the symptom pattern.
- Manual therapy: Hands-on work can improve wrist and forearm mobility and reduce strain in nearby tissue.
- Strengthening: Once symptoms calm down, targeted loading helps restore function.
- Ergonomic coaching: This is often the difference between short-term improvement and repeated flare-ups.
Some clinics also use supportive modalities as part of a broader plan. For example, iontophoresis in physical therapy may be considered in certain rehab settings when a clinician is trying to calm irritated tissue without relying only on oral medication.
Corticosteroid injections
Corticosteroid injection is one of the most established professional nonsurgical options for carpal tunnel. It works by reducing inflammation and swelling inside the carpal tunnel, which can temporarily reduce pressure around the nerve.
According to a PMC review of local corticosteroid injection for carpal tunnel syndrome, corticosteroid injections provide short-term relief for approximately 3 months on average, with high efficacy and safety in mild to moderate cases.
That makes injections useful in a few situations:
| Approach | What it helps with | Main limitation |
|---|---|---|
| Corticosteroid injection | Symptom reduction when pain, numbness, or night waking is limiting daily life | Relief is often temporary |
| Therapy-based rehab | Daily mechanics, nerve mobility, strength, and task modification | Requires follow-through and consistency |
An injection can calm things down enough for someone to sleep, function, and participate in rehab more effectively. But if nothing changes in hand use, work setup, or mechanics, the same forces may provoke the nerve again.
Other clinic-based care
Some patients also pursue acupuncture, chiropractic treatment, or shockwave therapy as part of a broader conservative plan. These approaches may help with pain control, soft tissue irritation, joint mechanics, or movement tolerance in selected cases.
The important point is to judge any option by a practical standard: does it improve symptoms and help you function with less nerve irritation, or does it only provide a brief reduction in discomfort? That question keeps treatment focused.
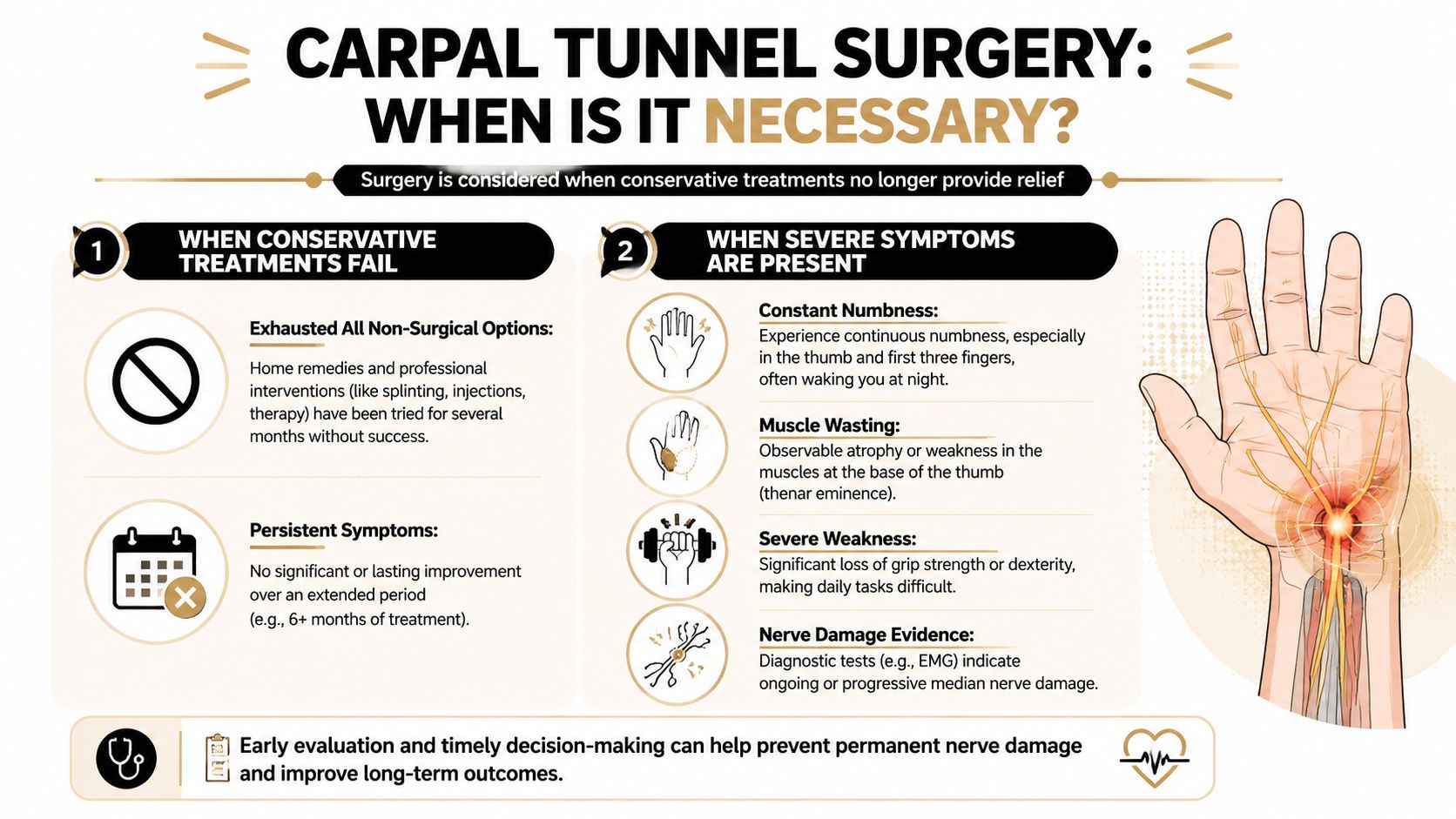
When Is Carpal Tunnel Surgery Necessary
Surgery enters the conversation when symptoms are more advanced or when a solid trial of conservative care hasn't been enough. It can also become the right choice sooner if testing shows significant nerve involvement or if there are signs of muscle wasting at the base of the thumb.
The basic goal of surgery
Carpal tunnel release surgery works by cutting the transverse carpal ligament. That increases space in the tunnel and relieves pressure on the median nerve. For moderate to severe carpal tunnel syndrome, it is considered the definitive treatment.
The summary published by Practice Plus Group on carpal tunnel surgery success rates states that surgical carpal tunnel release has a success rate exceeding 90% in relieving median nerve compression symptoms. The same source notes that surgery is generally reserved for people who haven't responded to an initial 6 to 12 week trial of conservative care, or for those with severe evidence of nerve damage.
Open release versus endoscopic release
The two main surgical approaches are open release and endoscopic release.
- Open release: A small incision is made in the palm so the surgeon can directly divide the ligament.
- Endoscopic release: Smaller incisions and a camera-guided approach are used to release the ligament from inside.
Both procedures aim to solve the same problem. The best approach depends on the surgeon's judgment, the patient's anatomy, and the overall clinical picture. What matters most is proper diagnosis and appropriate timing.
Surgery makes the tunnel larger. It doesn't erase the need to restore hand strength, movement, and function afterward.
When not to delay
Certain symptoms should push you to seek prompt medical evaluation:
- Constant numbness: Not just occasional nighttime tingling.
- Thumb weakness: Trouble with pinching, buttoning, or gripping.
- Visible muscle loss: Shrinkage at the base of the thumb.
- Progressive dysfunction: Daily tasks are getting harder, not just more uncomfortable.
Preoperative electrophysiological testing is typically used to confirm the need for surgery and document the severity of nerve compression. That's an important step, because it helps separate true carpal tunnel from other conditions that can mimic it.
Choosing Your Path and What to Expect
You wake up with a numb hand, shake it out, and tell yourself to wait another week. Then another. That is how mild carpal tunnel often turns into a bigger disruption. The right next step depends on symptom pattern, hand function, and whether the problem is calming down or steadily taking over more of your day.
I tell patients to choose treatment based on what the approach is designed to change. Splints and medication may reduce irritation for a while. They do not correct the repeated wrist positions, gripping habits, workstation setup, or loading patterns that often keep compressing the nerve. If the mechanics stay the same, symptoms often return.
A practical way to decide
Occasional nighttime tingling calls for a simple, focused plan. Start by changing the activities and positions that trigger symptoms, especially prolonged wrist bending, forceful gripping, and sustained pressure through the palm. A night splint can help if sleep is the main problem, but it works best as support for behavior change, not as the whole treatment.
If symptoms keep showing up during the day, interrupt work, or make household tasks less reliable, stop guessing. That usually means the problem needs a more structured exam and a treatment plan that addresses both symptom control and the reason the nerve keeps getting irritated.
What recovery usually looks like
Recovery is rarely one straight line.
A splint may settle night symptoms fairly quickly when wrist position is the main driver. An injection may calm pain and tingling faster than exercise-based care, but that benefit can fade if the wrist is still being loaded the same way every day. Therapy takes more participation, but it gives you a better chance to improve nerve mobility, tendon movement, grip tolerance, and hand use in real tasks.
As symptoms settle, some people need graded strengthening to rebuild capacity without flaring the hand. In that phase, hand exercise putty for grip and dexterity training can be useful as part of a guided program, not as a random add-on.
Surgery changes the space around the nerve. Recovery after surgery still depends on how irritated the nerve was beforehand, how stiff or weak the hand became, and how well you restore motion and function afterward. Relief from night numbness can come early, while strength and fine motor control often take longer.
Good treatment choices are not about doing more. They are about matching the plan to the stage of the problem.
Red flags that deserve immediate attention
Get prompt medical evaluation if you notice:
- Sudden loss of feeling
- Visible wasting at the thumb base
- Rapidly worsening weakness
- Progressive loss of fine motor control
Those changes suggest the median nerve may be under significant stress, and waiting can make recovery slower and less complete.
Find Your Partner in Recovery at MedAmerica Rehab
Carpal tunnel can feel confusing because so many treatments get lumped together as if they all do the same thing. They don't. Some reduce symptoms for a while. Some improve mechanics. Some are appropriate only after other measures fail. The best decisions come from understanding where your symptoms are now and what the treatment is designed to change.
An active approach usually gives people the clearest path forward. That means changing aggravating positions, improving nerve and tendon movement, restoring strength carefully, and escalating care when the situation calls for it. If surgery becomes necessary, rehab still matters because your hand needs mobility, strength, and coordination after the compression is relieved.
At MedAmerica Rehab Center, patients can be evaluated for a personalized plan that may include physical therapy, chiropractic care, acupuncture, advanced shockwave therapy, or post-surgical rehabilitation, depending on the presentation and goals. The point isn't to force one treatment on everyone. It's to match the treatment to the problem.
If your hand is tingling at night, going numb during the day, or losing strength, don't keep guessing. Contact MedAmerica Rehab Center to schedule an evaluation and get a clear plan for relief, function, and recovery.