Arthritis Pain Relief Prescription: A Patient’s Guide
You wake up already negotiating with your body. Your hands feel stiff around the coffee mug. Your knee complains when you step off the curb. Your back and hips need a few extra minutes before they trust you enough to move normally. By lunchtime, you may be asking the same question many people ask: do I need a prescription, and if I do, which one helps?
That question gets complicated fast. Some medications are meant to calm pain for a few hours. Others target inflammation. Some are used when the problem is wear-and-tear arthritis. Others are meant for autoimmune arthritis, where the immune system is part of the problem. Then there's the part many people don't hear clearly enough: medication can help, but it usually works best as one piece of a bigger plan that also improves strength, joint motion, balance, and daily function.
As a physical therapist would explain it, the goal isn't to lower pain on paper. Instead, the goal is to help you walk, sleep, bend, grip, climb stairs, and get through your day with less strain. An arthritis pain relief prescription can support that. It usually can't do the whole job by itself.
When Arthritis Pain Disrupts Your Life
Many people reach treatment after months of trying to push through. At first, it's small. You avoid the longer grocery route because your knee swells afterward. You stop gardening because your fingers ache for hours. You sit down to rest, then notice it hurts to stand back up.
That pattern wears people down emotionally as much as physically. Arthritis pain doesn't just hurt. It interrupts routine, confidence, and independence. When that happens, it makes sense to look at prescription options, especially if over-the-counter medicines, rest, or home remedies haven't done enough.
Prescription pain treatment is also common. National U.S. survey data from 2015 to 2018 showed that 10.7% of adults age 20 and older used one or more prescription pain medications in the past 30 days, and use increased with age and was higher among women than men according to the CDC data brief on prescription pain medication use. Those patterns overlap with who often struggles most with arthritis symptoms.
That doesn't mean everyone with arthritis needs medication. It does mean you're not unusual if you've reached the point of asking about one.
What patients usually want
The focus isn't on a perfect diagnosis term. Practical relief is what's desired:
- Morning movement that feels less guarded
- Enough comfort to work, cook, or drive
- Better sleep without waking from joint pain
- A plan that doesn't leave them dependent on pills alone
Arthritis care works better when the treatment plan matches the job you need your body to do.
A prescription can reduce pain enough for you to participate in exercise, physical therapy, or hands-on treatment. That matters. If pain is so high that you stop moving, joints often get stiffer, muscles weaken, and daily tasks become harder.
If you're sorting through options, a good starting point is understanding the broader picture of arthritis pain relief and conservative care. Medication makes more sense when you can place it inside a full plan instead of treating it like the entire answer.
Symptom Relief vs Disease Control
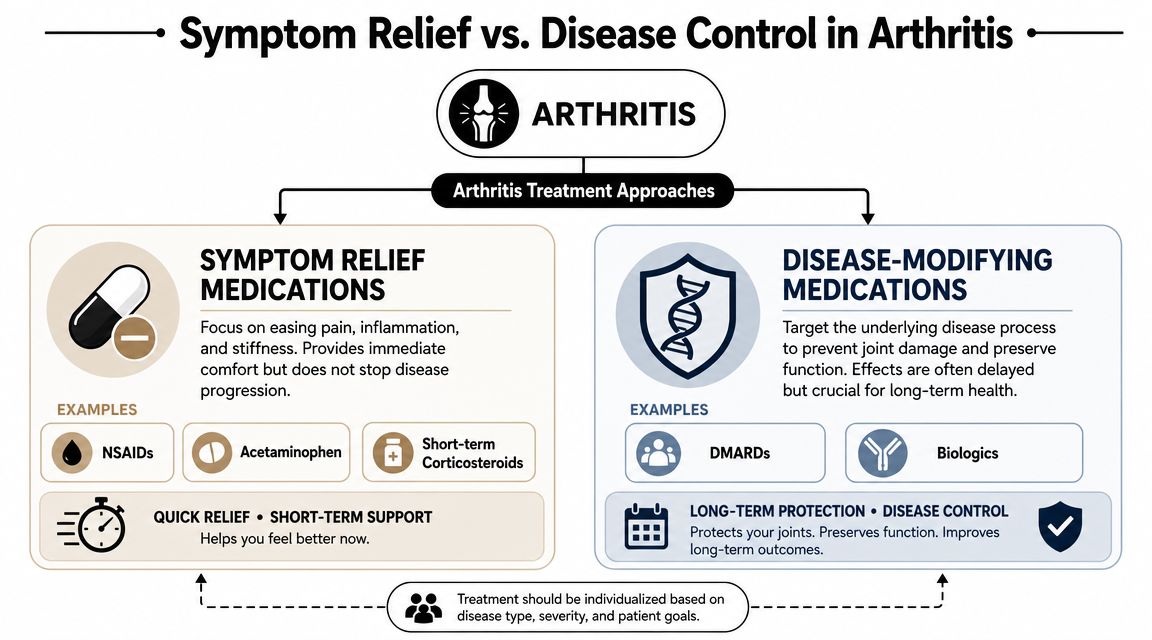
The biggest misunderstanding in arthritis treatment is that all arthritis medications do the same thing. They don't.
Some medications are built for symptom relief. They turn down pain, stiffness, and swelling. Others are used for disease control. They target the process that is damaging the joint over time.
The easiest way to think about it
If your smoke alarm is blaring, you can remove the battery and quiet the sound. That's symptom relief. Useful, sometimes necessary, but it doesn't put out the fire.
Disease control is putting out the fire.
That distinction matters because NSAIDs and corticosteroids mainly reduce pain and inflammation, while DMARDs such as methotrexate are used to slow rheumatoid arthritis progression and prevent joint damage as described in the PMC review on rheumatoid arthritis treatment goals.
Why the diagnosis changes the prescription
With osteoarthritis, the main issue is usually joint degeneration, load, irritation, and inflammation around the joint. The medication conversation often centers on pain control and improving function.
With rheumatoid arthritis and other inflammatory arthritis conditions, pain is only part of the story. If the immune process stays active, joint damage can continue even on days when pain seems partly controlled. That's why someone with RA may need a disease-modifying prescription even if a pain reliever takes the edge off.
Here's the practical takeaway:
- If the goal is getting through a painful flare, symptom relief may be the short-term priority.
- If the goal is protecting joints over time in inflammatory arthritis, disease control becomes central.
- If both are happening, a doctor may use more than one type of treatment at once, with each medication doing a different job.
Practical rule: Ask your prescriber, “Is this medicine meant to help me feel better, control the disease, or both?”
That one question clears up a lot of confusion. It also helps set realistic expectations. A pain reliever may help quickly but won't necessarily change the course of inflammatory arthritis. A disease-modifying drug may be essential long term but may not feel dramatic right away.
When patients understand that difference, they usually make better decisions and feel less discouraged when one medication helps pain but not function, or protects joints but doesn't immediately erase symptoms.
A Guide to Arthritis Prescription Medications
The phrase arthritis pain relief prescription covers several very different medication groups. The right fit depends on the type of arthritis, where the pain is located, how intense symptoms are, what other health conditions you have, and whether the main goal is short-term comfort or long-term control.
For osteoarthritis, guidelines support oral NSAIDs as the most effective first-line analgesic class, while topical NSAIDs are often recommended first for localized pain because they provide anti-inflammatory effect with lower systemic exposure, according to the Arthritis Foundation guide to osteoarthritis pain medications. For inflammatory arthritis like RA, medications such as DMARDs and biologics are used because they suppress the immune process.
Comparing Arthritis Prescription Medications
| Medication Class | How It Works | Primarily Used For | Key Considerations |
|---|---|---|---|
| NSAIDs | Reduce pain and inflammation | Often used for osteoarthritis and flare-related symptom relief | Can help pain and swelling, but they don't change the course of inflammatory arthritis |
| COX-2 inhibitors | A type of anti-inflammatory medication designed to reduce pain and inflammation | Often considered when an anti-inflammatory is needed | Still requires a medical review of risks, other medications, and overall health history |
| Corticosteroids | Rapidly reduce inflammation | Short courses for flares, or injections for targeted relief | Helpful for short-term control, but not usually a long-term standalone plan |
| DMARDs | Modify the underlying inflammatory disease process | Rheumatoid arthritis and other inflammatory arthritis conditions | Aimed at slowing progression and protecting joints, not just easing pain |
| Biologics | Target specific immune pathways involved in inflammation | Inflammatory arthritis when disease control is needed | Require close medical supervision and are used for disease management rather than simple pain relief |
What each class means in real life
NSAIDs are often what patients think of first. They can make it easier to walk, grip, or get through the day when an irritated joint is limiting movement. In osteoarthritis, that's often useful because the medication helps with both pain and inflammation.
Topical anti-inflammatory treatment can be especially helpful when pain is localized, such as one knee or a hand joint. That's one reason many clinicians like to start there before moving to broader systemic treatment.
Corticosteroids can calm a flare quickly. That speed is why doctors use them, but the trade-off is that they're generally not something to lean on as the entire long-term plan. In rehabilitation, steroid delivery can sometimes intersect with local treatment approaches. If your provider recommends a targeted anti-inflammatory strategy, it helps to understand related options like the iontophoresis patch with dexamethasone, which is used in some rehab settings for localized inflammation management.
What works and what doesn't
What tends to work:
- Matching the medication to the arthritis type
- Using the lowest effective medication burden
- Reassessing when a drug helps pain but not function
- Combining medical care with exercise, mobility work, and joint protection
What usually doesn't work well:
- Using pain relief alone for inflammatory arthritis that needs disease control
- Expecting a prescription to fix weak muscles, poor joint mechanics, or stiffness from inactivity
- Staying on a medication plan that reduces symptoms but leaves you less active over time
Some people feel discouraged when a prescription helps but doesn't restore normal life. That's often because pain is only one part of the problem. Joint loading, muscle weakness, guarded movement, fatigue, and balance changes all influence how arthritis feels day to day.
The Role of Opioids and Managing Prescription Risks
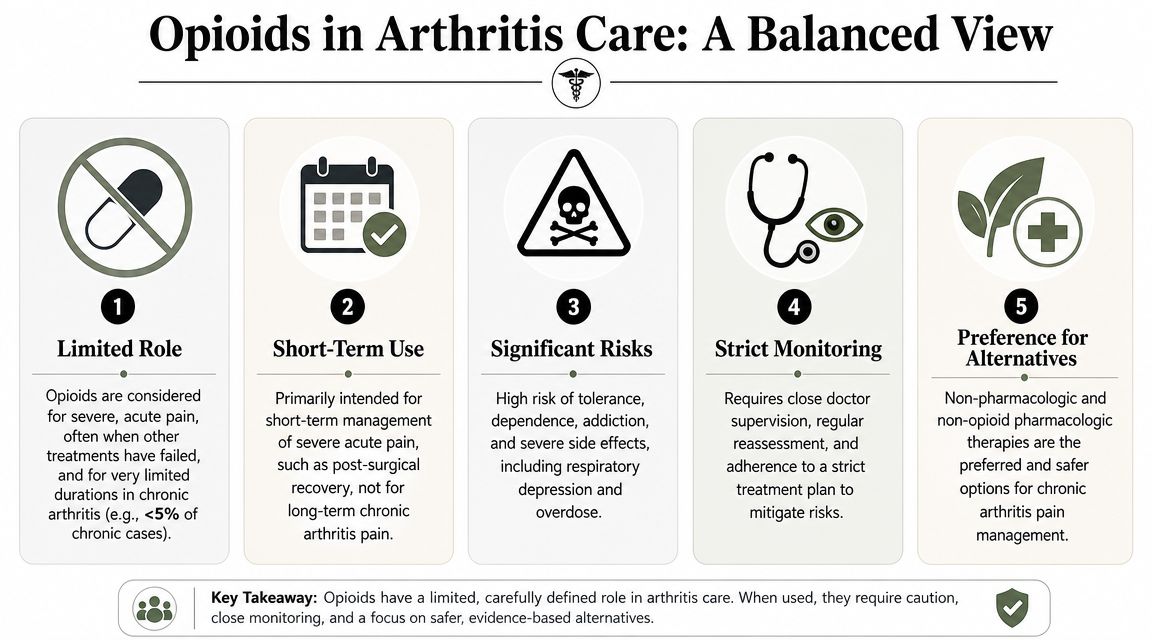
Opioids come up when pain has become severe, exhausting, or frightening. That conversation deserves honesty, not judgment.
For arthritis, opioids usually have a limited role. They may be considered in select situations, but they aren't the preferred long-term answer for most chronic arthritis pain. The reason is simple: while they may dull pain, they don't improve joint mechanics, they don't treat the underlying disease process, and they carry meaningful risks.
A major U.S. outpatient osteoarthritis study found 31,123 encounters over one year, and opioids or benzodiazepines were prescribed in nearly 27% of them, totaling 8,420 encounters in the PubMed study on prescribing in osteoarthritis. The same study reported that 43% of encounters involved patients age 65 or older, hydrocodone-acetaminophen was the most common medication prescribed at 34.3%, and 35.5% of patients had at least one risk factor for prescription misuse. The authors concluded that opioids and benzodiazepines remain commonly used despite evidence-based recommendations to the contrary.
Why doctors are cautious
Opioids can create a difficult trade-off. A patient may feel short-term relief, but over time the downsides can become hard to ignore:
- Sedation and slowed thinking
- Constipation and other side effects
- Tolerance, where the same dose seems less effective
- Dependence and difficult tapering
- Higher risk when combined with certain other medications
Severe pain is real. Caution around opioids isn't disbelief. It's an attempt to avoid creating a second problem while treating the first one.
If opioids are already part of your history
If you've been taking them, or you're worried about what happens when reducing them, that concern is valid. People often need support, education, and a medically guided plan rather than abrupt changes. A practical resource on managing opioid withdrawal can help you understand what symptoms may occur and why tapering should be supervised.
The broader goal in arthritis care is to reduce the need for opioid reliance by improving the things opioids can't fix: movement quality, joint support, pacing, strength, and inflammation management through safer long-term strategies.
How to Partner With Your Doctor for Safe Treatment
The safest arthritis prescription plans are collaborative. Patients do better when they speak up, keep track of what they're taking, and ask direct questions before a new medication starts.
A rushed appointment can make it feel like your only job is to nod and remember the pharmacy name. It's not. Your job is to understand what the medication is supposed to do, what it won't do, and how you'll know whether it's worth continuing.
Questions worth asking out loud
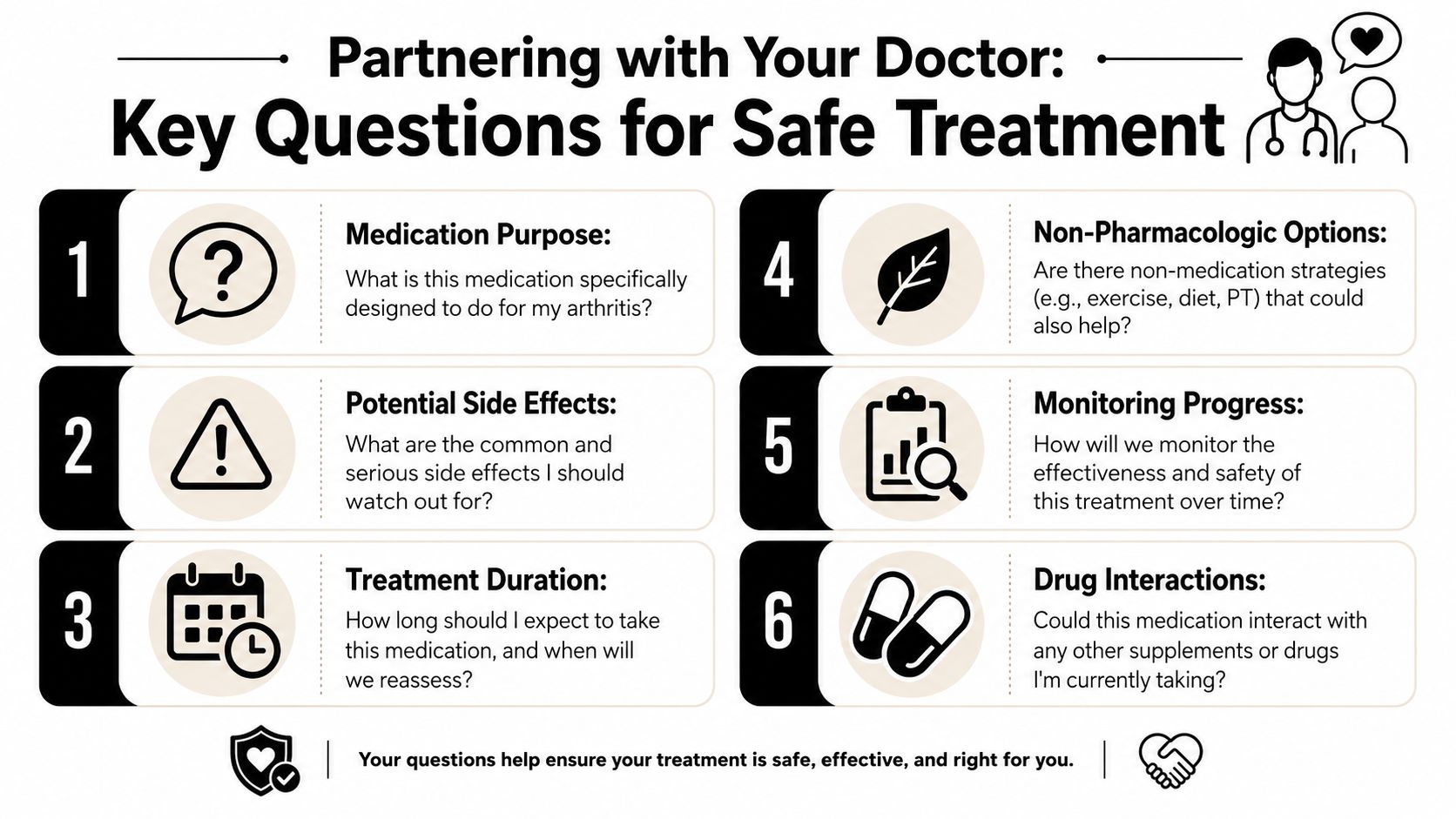
Bring these to the visit, or write them in your phone before you go:
What is this medication meant to do for me?
Pain relief, inflammation control, disease control, or some combination?How long should I take it before we judge whether it's helping?
Some medications are quick-acting. Others are not.What side effects should make me call the office?
“Common” and “serious” are not the same thing.Could this interact with my other prescriptions, supplements, or over-the-counter medicines?
This includes sleep aids, cold medicine, and anti-inflammatory products you may not think to mention.What's the plan if this doesn't help enough?
You want the next step, not just the first step.What else should I be doing besides taking the prescription?
Exercise, weight-bearing modifications, hand protection strategies, sleep position changes, and rehab all matter.
Keep one medication list
A simple written list can prevent a lot of trouble. Include:
- Drug names and doses
- How often you take them
- Why you take them
- Any side effects you've noticed
- Supplements and nonprescription products
Bring the list to every visit. Don't rely on memory when pain, stress, and multiple appointments are already competing for your attention.
Practical insurance frustrations
Insurance can complicate arthritis care, especially when prior authorization or step therapy is involved. If a prescription is delayed, ask these questions:
- Is there a covered alternative while approval is pending
- Does the office need any paperwork from me
- Would a different formulation be easier to approve
- Should I follow up with the pharmacy or the prescriber first
Patients often assume a delay means denial or that nobody is working on it. Sometimes it means the office and pharmacy haven't connected yet. A quick call can clear that up.
The best treatment plans are rarely passive. When you understand the purpose of the medication and your role in monitoring it, treatment gets safer and usually more effective.
Building a Life with Less Pain and Fewer Pills
Medication can calm symptoms. It can't teach a stiff hip to move better, strengthen a weak quadriceps, improve balance after knee pain, or correct the way you've started guarding one side of your body.
That's why long-term arthritis care works best when prescriptions are paired with non-pharmacologic treatment.

What rehab adds that medication can't
A person with knee arthritis may take an anti-inflammatory and feel some relief. But if they still have poor hip control, limited ankle motion, and weakness when stepping down stairs, the knee keeps absorbing stress in the same pattern.
That's where physical therapy changes the picture. It can help by:
- Improving joint motion so movement feels less blocked
- Strengthening the muscles around painful joints so the joint isn't doing all the work
- Training better movement mechanics for walking, stairs, lifting, and transitions
- Reducing fear of movement so people stop shrinking their lives around pain
Chiropractic care may help selected patients when spinal or joint mobility restrictions are contributing to stiffness and altered mechanics. Hands-on care, guided exercise, and progressive loading often work better together than any one of them works alone.
Think in terms of load, not just pain
Pain is what gets your attention. Load is often what keeps the problem going.
If a joint is irritated, your plan needs to reduce harmful load while building tolerance for healthy load. That may mean temporary activity modification, better footwear, mobility work, strengthening, and pacing. It may also mean changing how you return to hobbies.
For active adults, the same principle applies in recreation. Someone who loves golf may need more than a pill for post-round back or hip pain. They may benefit from movement coaching, trunk and hip conditioning, and swing adjustments. Practical advice like these tips for golfers with back pain can be useful when arthritis overlaps with sport and repetitive movement.
A structured rehab plan such as physical therapy for arthritis can fit into that broader approach by addressing stiffness, weakness, gait changes, and painful movement patterns that medication alone won't correct.
The best medication plan is often the one that creates enough breathing room for you to rebuild function.
A short visual overview can help if you're deciding whether movement-based care belongs in your plan:
What sustainable relief usually looks like
It usually isn't dramatic. It's practical.
You notice you're less stiff when you first stand up. You can open jars more easily. You stop planning your day around where you can sit down. Your flare-ups may still happen, but they don't own the whole week.
That's the value of a toolbox approach. Prescription medication may be one tool. Exercise is another. Manual therapy, pacing, sleep support, activity modification, weight management, and targeted strengthening all have their place. Relief becomes more durable when several parts of the plan support each other.
Your Next Step for Arthritis Relief in Deerfield Beach
If you're trying to decide whether an arthritis pain relief prescription is right for you, start with a simple question: what problem are you trying to solve right now?
If the issue is a painful flare that's limiting sleep or movement, symptom relief may be appropriate. If the issue is inflammatory arthritis that threatens long-term joint health, disease control becomes more urgent. If the issue is that pain keeps returning because your body has gotten weaker, stiffer, or less tolerant of activity, medication alone probably won't be enough.
That's where a combined plan makes the most sense. Good arthritis care often blends medical treatment with movement-based treatment. One calms symptoms. The other helps you function better and depend less on temporary relief.
For people in Deerfield Beach, local care matters because consistency matters. It helps to have a team that can look at the whole picture, including pain patterns, walking tolerance, joint mobility, exercise capacity, and how your symptoms are affecting daily life. MedAmerica Rehab Center has served the community since 1995 with a non-surgical approach that includes physical therapy, chiropractic care, acupuncture, and shockwave therapy for patients who need a broader plan than medication alone.
You don't need to have everything figured out before getting help. You just need a starting point, especially if pain has started changing how you move, work, or live.
If arthritis pain is interfering with your routine, the next step is to get a plan that fits your diagnosis, symptoms, and goals. MedAmerica Rehab Center can help you explore conservative treatment options, understand how rehab fits alongside medical care, and build a path toward better movement with less day-to-day pain.