ACL Surgery Rehabilitation Protocol: Your Phased Guide
You're probably reading this with a brace on your leg, your knee still swollen, and a stack of discharge instructions that feel harder to follow than they should. Patients in the first days after ACL surgery often want one simple answer: “When will I be back to normal?” The better question is, “What does my knee need to do before I move to the next step?”
That shift matters. A strong ACL surgery rehabilitation protocol isn't built around crossing off weeks on a calendar. It's built around earning the next activity through motion, strength, control, and confidence. Some people hit early milestones quickly. Others need more time because of swelling, pain, a meniscus repair, or the way their quadriceps shuts down after surgery.
The safest recoveries happen when you stop treating rehab like a countdown and start treating it like a series of tests your body has to pass. That approach lowers frustration, reduces setbacks, and gives you a clearer path back to walking, training, and eventually sport.
Your Roadmap After ACL Surgery
The first stretch after surgery often feels confusing because your day is full of limits. Use the brace. Use the crutches. Don't twist. Don't do too much. Those instructions protect the graft, but they don't always tell you what progress should look like.
A modern ACL surgery rehabilitation protocol gives you a different lens. Instead of asking whether you're “at week 3” or “at month 4,” it asks whether your knee can fully straighten, whether swelling is under control, whether your gait looks normal, and whether your strength is coming back evenly.
Why criteria matter more than the calendar
Two patients can be the same number of weeks from surgery and have very different knees. One may walk smoothly with low swelling. The other may still have a stiff extension loss and a visible limp. Advancing both the same way is how people end up irritated, swollen, and discouraged.
What works better is a criteria-based model built around checkpoints like these:
- Motion first: Full knee straightening has to return early, because a knee that won't fully extend often creates long-term walking problems.
- Swelling under control: A puffy, irritated knee won't move or recruit the quadriceps well.
- Muscle activation: Your quad has to wake up before higher-level strengthening makes sense.
- Movement quality: A smooth walk matters more than quickly ditching crutches.
Your body doesn't care what week it is. It responds to load, healing, swelling, and the quality of the work you do.
That's why patient education matters as much as exercise. If you understand what each phase is trying to restore, you're more likely to do the right work consistently and less likely to push at the wrong time. If you want broader guidance on recovery after knee procedures, this overview of physical therapy after knee surgery is a useful starting point.
What to expect emotionally
There's also a mental side that generic protocols ignore. Early on, many patients are worried they'll bend too far, put too much weight through the leg, or damage the graft with routine movement. Later, that fear often changes shape. The knee may be stronger, but cutting, landing, or trusting the leg again can feel far harder than simple exercises did.
That's normal. Confidence doesn't show up all at once. It builds when your knee repeatedly proves it can handle the next task.
Phase 1 The First Weeks of Protection and Motion
The first phase is quiet work, but it has outsized consequences. If you do this part well, the rest of rehab tends to go smoother. If you rush it, the knee often reminds you quickly with more swelling, poorer motion, and a stubborn limp.

The non-negotiables early on
In this phase, the main priorities are simple and specific. Phase 1 focuses on restoring full knee extension (0°), eliminating joint effusion, and achieving active quadriceps contraction without lag. Progression criteria are tied to these goals, with modalities like controlled leg press at 50% body weight and backward treadmill walking used to prepare for Phase 2 according to Team ACL's rehabilitation guidance.
Those three targets drive almost everything you do in the first weeks:
- Get the knee fully straight: This is often harder than patients expect, and it's one of the most important early wins.
- Calm the swelling: If the joint stays irritated, motion and muscle recruitment both lag behind.
- Wake up the quadriceps: Your quad often feels disconnected after surgery. Re-establishing that contraction is a major milestone.
What your home routine usually centers on
Most early exercise programs are intentionally basic. That doesn't mean they're optional.
A typical early routine often includes:
- Quad sets: Tighten the front of the thigh and press the knee toward straight. This is how you start rebuilding the brain-to-muscle connection.
- Heel slides: These help restore bending without forcing it.
- Calf pumps and ankle movement: Useful for circulation and for limiting stiffness from being less active.
- Heel prop or supported extension work: This helps the knee settle into full straightening.
- Short, controlled walking practice: Only if your surgeon and therapist allow it, and only with good mechanics.
If you need examples of gentle mobility work, these range of motion exercises can help you understand the difference between productive stretching and forcing the joint.
Practical rule: Don't judge an exercise by how hard it feels. Judge it by whether it improves swelling, extension, quad control, and walking quality.
What patients often get wrong
The biggest mistake is doing too much on a knee that's still reactive. More standing, more walking, and more “testing it out” often lead to more fluid in the joint. Then the quad shuts down again, and the knee gets stiffer.
The second mistake is chasing bend while ignoring straightening. Patients notice flexion because it's easier to see. Extension loss is less dramatic, but it's often more disruptive to walking and long-term knee mechanics.
A few signs you're moving in the right direction:
| Early checkpoint | What it should look like |
|---|---|
| Extension | Knee gets fully straight without a painful struggle |
| Effusion | Swelling gradually settles instead of increasing day by day |
| Quad control | You can tighten the quad and lift the leg without the knee sagging |
| Walking | Weight bearing becomes smoother, not more protective |
The psychological piece in Phase 1
This phase can feel slow because the exercises don't look athletic. That can be frustrating, especially for active patients who are used to measuring progress by sweat and intensity.
Early confidence comes from seeing small things improve. The first solid quad contraction matters. The first smoother walk to the bathroom matters. The first time your knee lies flat and straight on the table matters. Those aren't minor details. They're the foundation of everything that comes next.
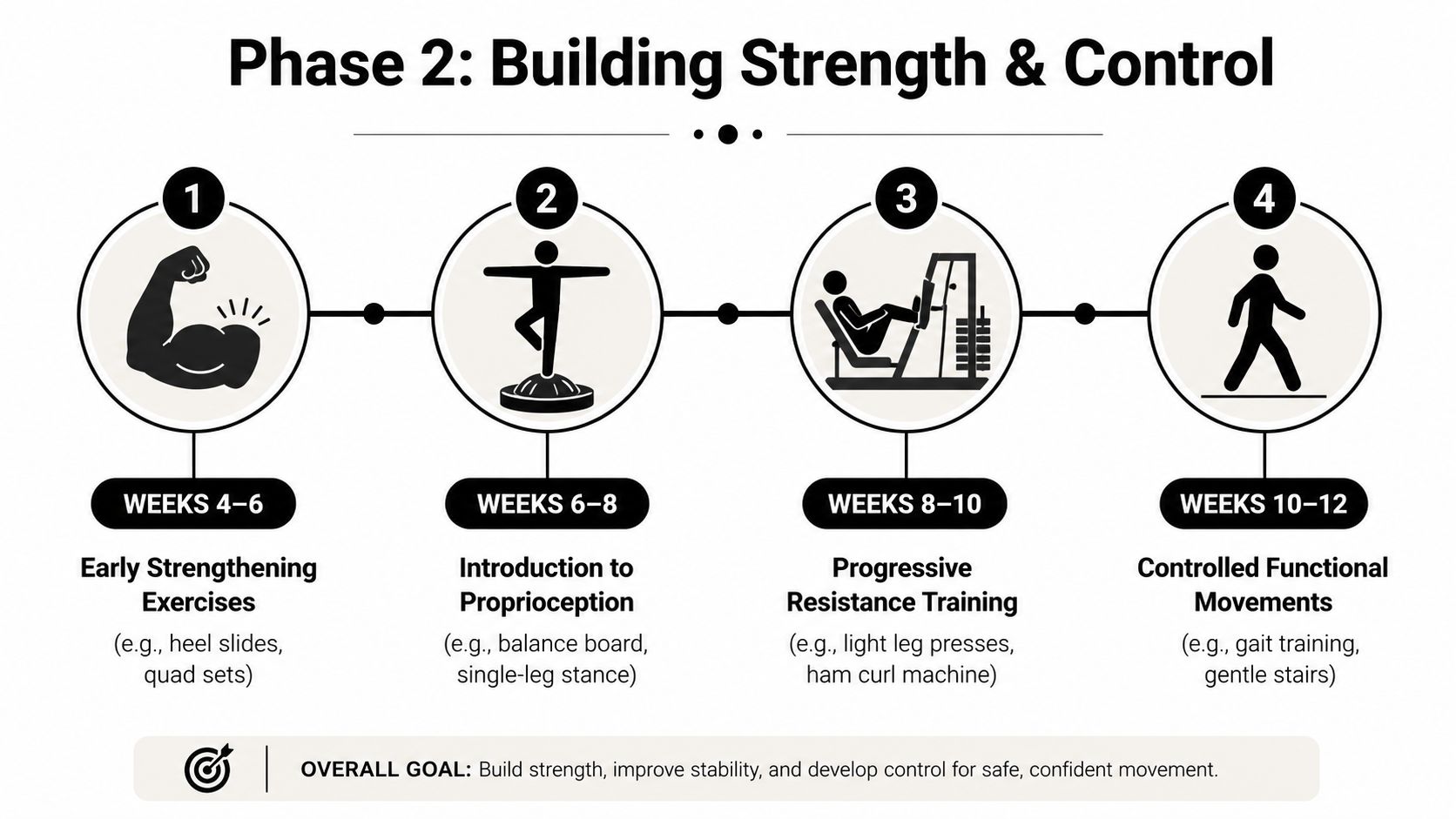
Phase 2 Building a Foundation of Strength and Control
There's a point when rehab shifts from protecting the knee to rebuilding the person attached to it. You're not just trying to reduce symptoms anymore. You're trying to create a leg that can accept load, hold alignment, and move without hesitation.
Walking normally is a strength milestone
Many patients think getting rid of crutches is mostly about time. It isn't. It's about whether you can walk without a limp, fully load the leg, and control the knee in stance.
Evidence-based protocols show that patients can walk without crutches in 2 to 6 weeks and ride an exercise bike in 3 to 4 weeks. The same guidance also supports starting early open kinetic chain exercises from 90° to 45° flexion at 4 weeks to accelerate quadriceps recovery without harming the graft, based on Aspetar's rehabilitation recommendations.
That matters because the quadriceps is usually the muscle group that lags the most after ACL reconstruction.
Closed chain and open chain both matter
Patients often hear that closed-chain work is “safe” and open-chain work is “risky.” That's an outdated oversimplification.
Here's the practical view:
| Exercise type | Examples | Why it matters |
|---|---|---|
| Closed-chain | Squats, leg press, sit-to-stand, step work | Builds whole-leg control in weight bearing |
| Open-chain | Carefully prescribed knee extension work in approved ranges | Helps target the quad directly when it's still weak |
Closed-chain work teaches the leg to work as a system. Open-chain work gives you a way to isolate a muscle that often won't fully recover if you only squat and step. A lot of patients can “hide” quad weakness during functional movements by shifting, shortening the stance phase, or relying on the other side.
That's why stronger rehab plans don't make this an either-or debate.
What progression often looks like in practice
This middle phase usually includes a blend of strength, balance, and movement retraining. The details vary, but common progressions include:
- Bike work: Useful for motion, circulation, and reintroducing rhythmic knee movement.
- Leg press and squat patterns: These help load the knee gradually in a predictable way.
- Step-ups and controlled stair work: Good for rebuilding daily function.
- Single-leg balance drills: These expose shaky control quickly.
- Hamstring and calf strengthening: Important for knee support and lower-leg control.
A knee that's ready for more work usually shows it with better tolerance, not bravado. Swelling stays manageable. Your gait stays clean. The knee doesn't get noticeably angrier the day after training.
Some soreness after a strengthening day can be normal. A big jump in swelling, limping, or loss of motion means the load was too much or progressed too fast.
Confidence starts to catch up here
This is often the phase where patients feel the first real sense of momentum. You can do more. You're less dependent on crutches and the brace. Everyday tasks stop feeling like a production.
But this is also when fear can become sneakier. A patient may look better physically but still unload the surgical leg during stairs, sit-to-stand, or mini squats. That hesitation is useful information. It tells you confidence hasn't caught up to capacity yet.
A good therapist doesn't just load the leg harder. They make the movement repeatable enough that your brain starts trusting it again.
Phase 3 Advanced Training and Neuromuscular Control
This phase starts to feel less like recovery and more like preparation. Strength still matters, but strength alone won't protect your knee when you have to absorb force, change direction, or react quickly.
That's where neuromuscular control becomes central. Your brain has to recognize position, coordinate timing, and recruit the right muscles fast enough to keep the knee in a good path. If you want a clearer picture of that process, this explanation of neuromuscular reeducation lays out why it's such a big part of orthopedic rehab.
Running is earned, not scheduled
A lot of patients circle the date they hope to jog again. The knee doesn't care about the date. It cares whether it can tolerate impact.
For this stage, the criteria are specific. Progression to running drills requires a minimum 70% quadriceps and hamstring Limb Symmetry Index on isokinetic testing. Agility drills only begin after achieving 85% symmetry, according to Jeremy Burnham MD's ACL recovery timeline.
Those thresholds matter because running and agility expose the knee to very different loads than biking or squatting.
What advanced training usually includes
At this stage, sessions become more movement-driven. Common categories include:
- Landing mechanics: Double-leg landings first, then more demanding variations as control improves.
- Deceleration drills: Slowing down cleanly is as important as speeding up.
- Single-leg strength work: This shows whether the surgical side can adequately carry its share.
- Change-of-direction prep: Start with simple, predictable patterns before sport-specific movement.
- Hop and rebound drills: Only when the knee demonstrates solid alignment and quiet landings.
One thing I tell patients often is that noisy landings usually mean poor force control. If your foot slaps down, your trunk wobbles, or your knee dives inward, the body is telling you the task is still ahead of your current control.
Quality beats intensity
Athletes sometimes sabotage themselves. They feel stronger, so they chase fatigue instead of precision. That's not the target. A poorly controlled jump is not a stepping stone to a better one. It's rehearsal for the wrong pattern.
Use a simple checklist during advanced drills:
- Can you hold alignment? The knee shouldn't collapse inward.
- Can you absorb force smoothly? Landings should look controlled, not jarring.
- Can you repeat it consistently? One good rep doesn't mean the pattern is reliable.
- Does the knee stay calm afterward? Swelling and reactivity still matter.
If your confidence drops every time the drill gets faster, the answer usually isn't “push through.” The answer is to scale the task until form and trust return together.
The mental side becomes more obvious here
Fear of re-injury tends to show up most clearly when impact and unpredictability return. A patient may be strong on testing but still hesitate before a jump or cut. That hesitation isn't weakness. It's part of recovery.
The best way through it is graded exposure. Start with drills that feel manageable. Repeat them until they feel boring. Then add speed, complexity, or reactivity one layer at a time. Confidence grows when the knee repeatedly handles a challenge without a bad consequence.
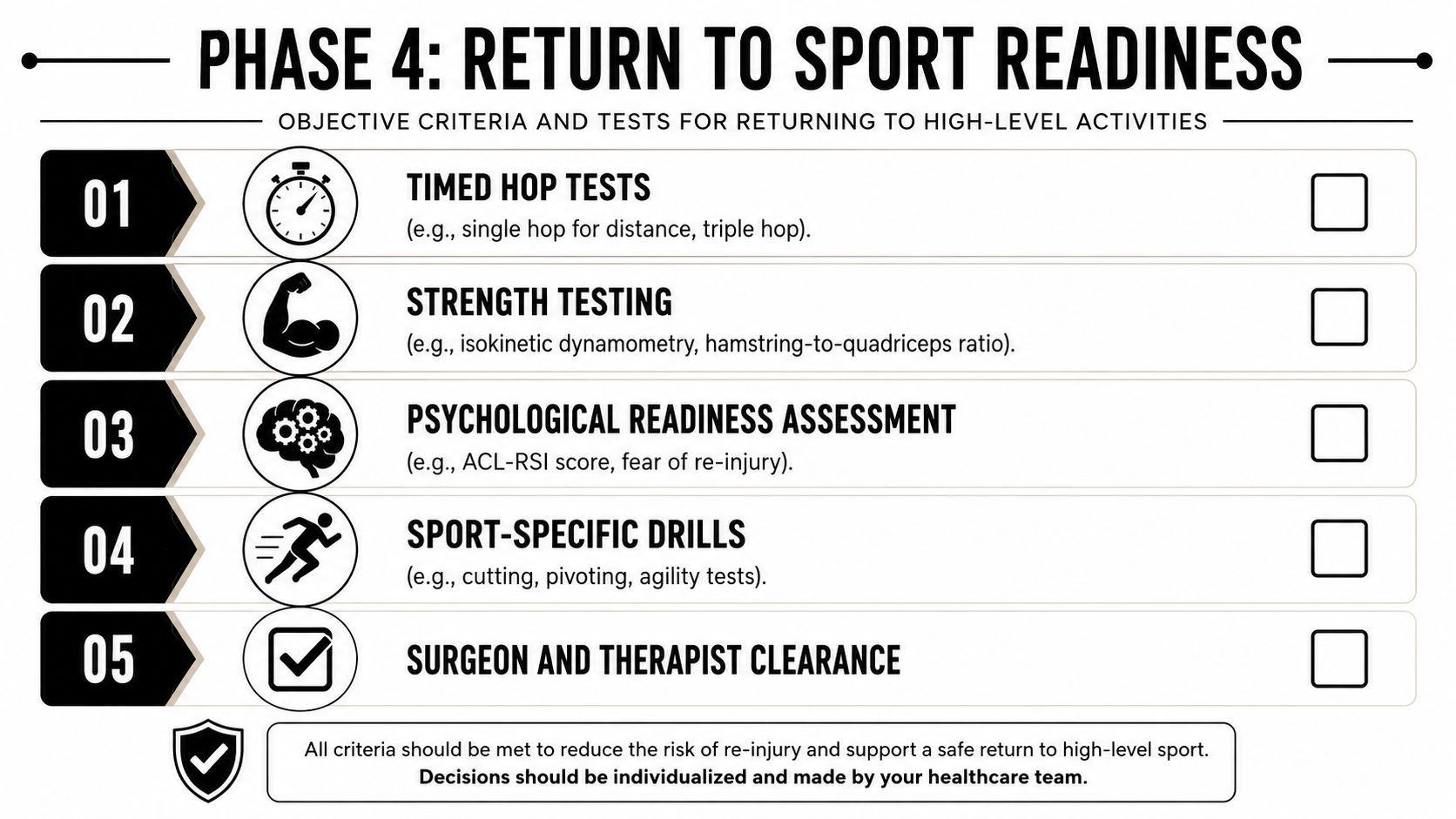
Phase 4 The Final Hurdles and Returning to Sport
Clearing someone for unrestricted sport should never be a casual decision. The knee has to pass a full return-to-sport exam, and that exam has both physical and psychological parts.
Current guidelines strongly recommend avoiding return to sport for a minimum of 9 to 12 months after ACL reconstruction, and young athletes who return prematurely show a second ACL injury range of 23% to 36%. The same guidance also highlights criteria such as Limb Symmetry Index greater than 95% and an ACL-RSI score of at least 90% before return to sport is considered, as detailed in this review on return-to-sport decision making after ACL reconstruction.
That recommendation isn't just caution. It reflects graft healing, strength recovery, functional symmetry, and readiness under load.
A separate evidence summary also notes that athletes returning earlier face a re-injury rate as high as 36%, while those who meet biomarker criteria like at least 95% quadriceps strength symmetry and hop test symmetry have a 4 to 7 times lower reinjury risk, as described in this ACL rehabilitation protocol review.
What the final testing should include
A good return decision usually pulls from several buckets, not one test.
| Clearance area | What clinicians look for |
|---|---|
| Strength | Symmetry between sides, especially quadriceps and hamstrings |
| Hop testing | Distance, control, landing quality, and side-to-side symmetry |
| Movement quality | Cutting, decelerating, and absorbing force without breakdown |
| Psychological readiness | Confidence, fear level, and willingness to trust the leg |
| Sport-specific ability | Position-specific or activity-specific demands done at game speed |
Here's a useful visual summary of what that checklist can involve.
Why time alone is a poor clearance tool
Nine months on the calendar does not automatically mean the knee is ready. Some athletes still show obvious side-to-side asymmetry, guarded landings, or fear during cutting drills. Others are physically close but mentally hesitant. Both matter.
A patient who says “my knee feels fine” can still fail a hop test, unload during a jump, or tense up during a reactive drill. Those are not minor details. In pivoting sports, they're warning signs.
Return to sport isn't a date. It's a decision supported by testing, movement quality, and confidence under pressure.
Don't overlook recovery habits outside the clinic
By this point, training load, sleep, stress management, and nutrition all affect how well you tolerate the final push. For patients cleaning up recovery habits, practical nutrition resources can help. This guide on how plants enhance athlete performance is one example of a useful read for fueling training and recovery without overcomplicating the issue.
The best return is the one you can sustain. Not just the one you can survive for a week.
Navigating Your Recovery at MedAmerica Rehab
You leave surgery with a brace, a packet of instructions, and one question that shows up fast. "How do I know if I'm on track?" The answer is rarely found in a generic week-by-week chart. What matters is how your knee responds, what your movement looks like, and how much trust you have in the leg as activity builds.
Why one patient's timeline shouldn't become yours
Recovery after ACL reconstruction is shaped by details that matter. A meniscus repair can limit early loading or motion. A hamstring graft changes how we build strength compared with a patellar tendon graft. A patient who wants to get back to lifting and hiking does not need the same final phase as a soccer player who must cut, pivot, and react under pressure.
That is why strict timelines often create the wrong kind of pressure. Patients start comparing themselves to a chart or to a friend's recovery and miss the actual question. Is the knee ready for the next step?
In the clinic, I look for clear signs of readiness:
- How does the knee respond after loading? Swelling, soreness, and stiffness the next day tell us a lot.
- Is motion still improving? Full extension and usable flexion need to keep progressing.
- Can the quadriceps work without compensation? If the hip or the other leg is doing the job, strength numbers can be misleading.
- Does movement stay clean? Walking, squatting, landing, and direction changes should look controlled, not guarded.
- Is fear changing your mechanics? Hesitation is common, but it needs to be addressed, not ignored.
Confidence is part of the progression. A patient may be strong enough for a drill on paper and still protect the leg during a landing or cut. That patient is not ready for the next jump in demand yet.
Red flags that deserve quick attention
Some fluctuation is normal after ACL surgery. Some changes need a faster response.
Contact your surgeon or rehab team if you notice:
- Swelling that keeps building and does not settle with rest or activity changes
- Sharp pain, catching, or a blocked feeling during motion
- Loss of motion after the knee had been improving
- A limp that is getting worse instead of fading
- Fear that is strong enough to change how you move during basic tasks or rehab drills
The best rehab plan responds to those signs early. Pushing through them usually slows progress.
What skilled rehab should feel like
Good therapy should feel specific to you. Your therapist should measure the things that matter, explain why you are doing each exercise, and change the plan when the knee says it is not tolerating the current load. You should know what milestone you are working toward, whether that is full extension, better quad control, cleaner landing mechanics, or confidence during cutting.
At MedAmerica Rehab Center, care is built around presentation, not a generic calendar. The team works with post-surgical patients through hands-on treatment, targeted exercise progressions, and close tracking of motion, gait, strength, balance, and return-to-activity readiness. That matters because ACL recovery is rarely a straight line. Some weeks are about pushing. Some are about calming the knee down and restoring quality.
A strong result comes from matching the work to the stage of healing, then progressing when both the knee and the patient are ready.
If you're recovering from ACL surgery and want a personalized, criteria-based plan instead of a one-size-fits-all timeline, MedAmerica Rehab Center can help. Their team in Deerfield Beach works with post-surgical patients through each stage of recovery, from restoring motion and quad activation to advanced return-to-sport testing, so you can move forward with more clarity and confidence.