
Expert Tips: Exercise After Operation
You’re home after surgery. The hospital bracelet is off, the discharge papers are on the counter, and now the quiet question starts: How much should I move, and how much is too much?
It's natural to feel a mix of relief and uncertainty at this stage. You want to heal well. You also don’t want to do something that sets you back. That tension is normal, and it’s one of the biggest reasons exercise after operation should never mean “just push through it” or “stay in bed until everything feels normal.”
Done correctly, movement helps healing rather than interrupting it. It supports circulation, wakes muscles back up, reduces stiffness, and rebuilds confidence. It also gives recovery some structure, which matters more than people realize when every day feels different.
A plan matters before surgery and after it. Research summarized by Physio-Pedia on physical activity before and after surgery found that structured preoperative exercise interventions improve postoperative outcomes, and some studies showed high-intensity interval training reduced hospital stays by an average of two days for major abdominal surgery patients. The takeaway is simple: if targeted exercise helps patients go into surgery stronger, a targeted recovery plan helps them come out of it with fewer setbacks.
If you’re feeling unsure about what “starting again” should look like, a general fitness resource like how to start working out again can help frame the mindset. Post-op exercise is more medically specific, but the same principle applies. You rebuild in layers, not all at once.
If you’re preparing for therapy visits, it also helps to know what to expect at a physical therapy appointment. Knowing the process tends to lower stress, and lower stress often makes patients move better.
The First Steps Matter Most in Your Recovery
The first days after surgery often shape the rest of recovery. Not because everything has to go perfectly, but because early habits tend to stick. If you spend that window waiting for pain or stiffness to disappear before moving, it usually doesn’t work out that way. Gentle, guided activity is often what helps those symptoms begin to ease.
Why rest alone isn’t enough
Rest is necessary, especially for tissue healing and pain control. But complete inactivity can create new problems. Joints stiffen. Muscles switch off. Walking starts to feel awkward, then tiring, then intimidating.
That’s why exercise after operation isn’t about “fitness” in the usual sense. At first, it’s about restoring normal body functions:
- Circulation support: Small movements help blood flow and reduce the effects of lying or sitting too long.
- Breathing quality: Deep breathing and posture changes help you expand the lungs and reduce shallow, guarded breathing.
- Joint protection: Gentle motion keeps nearby joints from becoming unnecessarily stiff.
- Confidence: Each safe movement teaches your nervous system that activity is possible.
Practical rule: If an exercise is appropriate for your stage, it should challenge you a little, not alarm you.
What a good early plan feels like
A good plan doesn’t feel heroic. It feels repeatable. You know what movements to do, how often to do them, and what response is acceptable afterward. You don’t need to guess every day.
The patients who usually do best aren’t always the toughest. They’re often the ones who stay steady. They do the simple things well, they adjust when symptoms flare, and they ask for help before a small issue turns into a longer delay.
Navigating the Phases of Post-Operative Healing
Recovery is easier to manage when you stop thinking of it as one long stretch and start thinking in phases. The exercises that help in the first two days are not the same ones that help when you’re rebuilding endurance or getting back to work, golf, stairs, or driving.
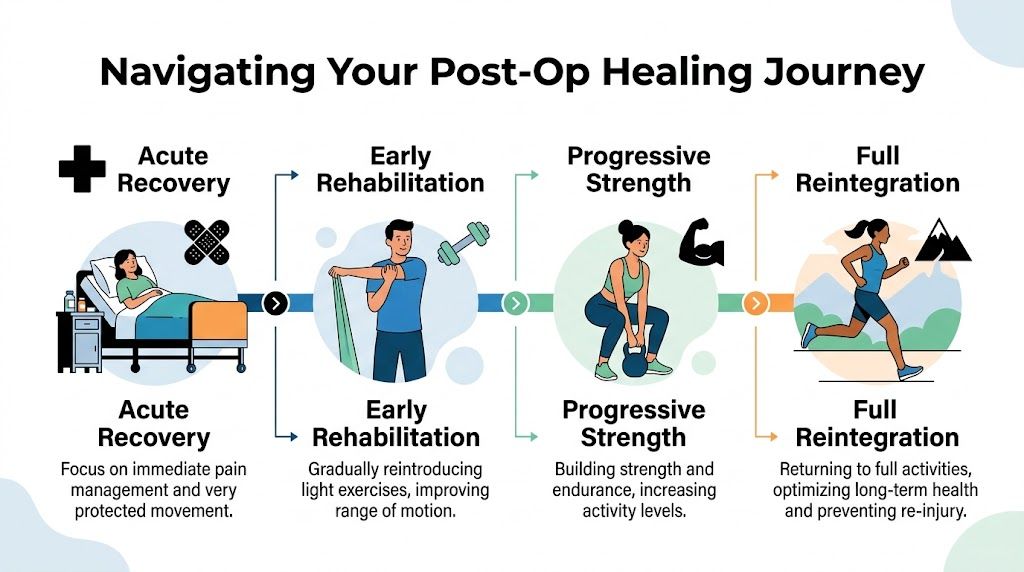
Phase 1 Acute recovery
In the immediate period after surgery, the main goals are protection, circulation, pain control, and safe basic movement. This stage is usually quieter than people expect. The right exercises often look small from the outside.
Enhanced recovery after surgery protocols support getting people moving early. According to this overview of post-operative mobility in ERAS protocols, mobilization begins within 24 hours with in-bed activities, then progresses to supervised short walks of 10 to 20 meters by postoperative day 1 to 2, with a goal of at least 500 steps per day to help reduce complications by 20 to 30%.
That early movement often includes:
- Ankle pumps: Useful when you’re not walking much yet.
- Heel slides: Helpful for gentle knee and hip motion if your surgeon allows them.
- Bed mobility practice: Rolling, scooting, and getting to the edge of the bed safely.
- Short assisted standing or walking: Not for speed. Just for tolerance and mechanics.
At this stage, patients often make one of two mistakes. They either do too little because they’re scared, or too much because they’re eager. Neither helps. A better target is “frequent and gentle.”
The first walk after surgery doesn’t need to look impressive. It needs to be safe enough to repeat later that day or the next.
Phase 2 Early rehabilitation
This phase usually centers on reintroducing regular movement into the day. You’re no longer just trying to get through transfers and short walks. Now the question becomes whether your body can tolerate repeated activity without swelling, sharp pain, or deep fatigue.
The focus shifts toward:
- Range of motion
- Basic muscle activation
- Walking pattern
- Simple daily tasks
Many patients often start bargaining with themselves. If they feel okay one morning, they try to catch up for lost time. Then they flare up at night and assume exercise is the problem. Often the issue isn’t exercise itself. It’s poor dosing.
A useful way to think about this stage is to compare activities by purpose:
| Activity | Best use | Common mistake |
|---|---|---|
| Short walks | Builds tolerance and confidence | Turning one good walk into an overlong session |
| Range-of-motion drills | Reduces stiffness and restores joint movement | Forcing the end range |
| Isometrics | Activates weak muscles with low joint stress | Holding breath during effort |
| Light functional tasks | Reconnects therapy to real life | Doing tasks with poor form because “it counts” |
Phase 3 Building foundational strength
Once swelling, pain irritability, and movement quality are more controlled, you can start building strength with more intention. This phase matters because daily life asks for repeated effort. Standing from a chair, climbing stairs, carrying groceries, and walking through a store all require endurance plus control.
Exercises here may include sit-to-stands, step work, standing hip work, gentle resistance band movements, supported balance drills, and low-load strengthening that matches your surgery and precautions. The key is quality. If the movement pattern falls apart, more reps won’t solve it.
Watch for these signs that you’re progressing well:
- You recover within a reasonable time after sessions
- Your walking becomes less guarded
- You need fewer compensations to complete normal tasks
- Your confidence rises along with your capacity
Phase 4 Returning to life’s activities
This phase is where exercise after operation becomes less about rehab and more about function. You’re no longer asking, “Can I do the exercise?” You’re asking, “Can I do my life again without paying for it afterward?”
That may mean returning to:
- Work demands
- Driving
- Household chores
- Reaching, lifting, or carrying
- Sports and recreation
This phase is also where many people need the most restraint. Pain may be lower, but tissue tolerance still has to catch up to your ambition. A patient can feel “mostly normal” and still overload a healing joint, tendon, or surgical area by jumping too fast into yard work, pickleball, or a long outing.
Recovery gets more durable when your exercise plan starts to resemble your real life. If stairs are hard, train stairs. If getting off the floor matters, practice that pattern safely.
Your Toolkit of Essential Post-Op Exercises
The best early exercises aren’t always the most exciting ones. They’re the ones that solve the problems surgery creates: shallow breathing, swelling, stiffness, muscle shutdown, and fear of moving.

Breathing and relaxation work
After surgery, people often brace without realizing it. They hold tension in the jaw, shoulders, abdomen, and hips. That guarding can make pain feel louder and movement feel harder.
Start with slow diaphragmatic breathing. Inhale through the nose if possible, let the lower ribs expand, then exhale without forcing it. If your surgeon has recommended cough support or breathing tools, follow that plan closely.
Why it matters:
- It improves chest expansion
- It reduces protective tension
- It can make transfers and walking feel less rigid
Circulation and motion drills
These are the classic early staples for a reason. Ankle pumps, heel slides, gentle knee bends, elbow bends, wrist circles, and short supported walks all help your body re-enter movement without large loads.
Patients sometimes dismiss these because they seem too easy. That’s backwards. If an exercise improves circulation, keeps a joint moving, and can be repeated several times a day, it’s doing important work.
Useful examples include:
- Ankle pumps while lying down or sitting
- Heel slides if allowed after your procedure
- Gentle seated marching for hip and trunk tolerance
- Shoulder pendulums when appropriate after shoulder procedures
If muscles feel tight and overworked around the surgical area, a clinician may later add recovery tools like guided soft tissue work or foam rolling to nearby regions. If you’re curious how that kind of self-care tool fits into rehab, this overview of a PE foam roller and how it supports movement work gives helpful context.
Isometric activation
Some muscles stop contributing well after surgery, even when you’re trying. Isometric work helps “wake them up” without asking the joint to move much.
Common examples are quadriceps sets, glute squeezes, and gentle abdominal bracing. These don’t look dramatic, but they often improve control faster than patients expect when done consistently.
A simple cue helps: tighten with intention, breathe normally, then release fully. Don’t clamp down so hard that the whole body tenses.
For a visual walkthrough of gentle early movement ideas, this video offers a useful starting point:
Early strength and balance
Once your therapist or surgeon clears you, you’ll usually add low-level strengthening and balance tasks. Sit-to-stands, weight shifts at the counter, mini step-ups, supported heel raises, and standing hip work are common choices.
Here’s what tends to work versus what usually doesn’t:
- What works: controlled reps, good posture, and stopping before your form breaks down
- What doesn’t: chasing muscle burn, moving too fast, or copying a stronger person’s program online
- What works: short sessions done consistently
- What doesn’t: one long “make-up workout” after skipping several days
Adapting Exercises for Your Specific Surgery
Two patients can both say, “I had surgery,” and need very different exercise plans. A knee replacement, hip replacement, rotator cuff repair, and lumbar procedure each place different limits on the tissues that are healing, the movements that are safe, and the patterns that need to come back first.

That difference matters for another reason. Fear of movement often shows up when patients are not sure what is safe for their specific surgery. Clear modifications reduce guesswork, and that usually helps people move with more confidence.
Knee and hip recovery
After knee surgery, the early job is usually to restore knee straightening, improve bending gradually, calm swelling, wake up the quadriceps, and clean up walking form. Many patients chase flexion because the stiffness feels obvious. Full extension deserves equal attention because even a small loss there can change gait, standing tolerance, and stair mechanics.
Hip surgery asks for a slightly different focus. Walking quality, safe transfers, glute activation, and respect for any surgical precautions matter early. I often remind patients that a strong leg can still move poorly if every step is practiced with a limp.
A quick comparison helps:
| Surgery | Helpful early focus | Common trap |
|---|---|---|
| Knee replacement | Quad sets, heel slides, gait practice, sit-to-stands | Ignoring full knee straightening |
| Hip replacement | Weight shifts, walking form, glute activation, transfer practice | Moving carelessly around precautions |
If arthritis is already part of the picture, the plan often needs more support. Shorter walking bouts, higher chairs, counter support, and slower sit-to-stands can keep the exercise productive without irritating the joint.
Shoulder and back procedures
Shoulder surgery recovery usually works best when patients protect healing tissue without letting the shoulder get unnecessarily stiff. Early exercises often include pendulums, scapular setting, hand and wrist motion, and then controlled range of motion as the repair allows. The common mistake is testing the shoulder because stiffness feels like a sign that more stretching is needed.
For rotator cuff repairs in particular, timing matters as much as exercise choice. This guide to effective home exercises after rotator cuff surgery gives a useful example of stage-appropriate progressions patients can follow at home.
Back surgery patients usually respond better to frequent short walks, position changes, gentle trunk control, and careful mechanics for bed mobility, sitting, and standing. Big stretches into pain often add guarding instead of helping. Controlled, repeatable movement usually gets better results.
A successful plan has to fit both the surgery and the person doing the work. The right program for an active worker is not always the right program for a retired adult managing arthritis, balance changes, or low stamina.
When arthritis or body weight changes the plan
Generic online routines often miss actual factors that shape recovery. Arthritis, reduced endurance, balance concerns, and higher joint load can all change what a good exercise session looks like. Those factors do not mean progress has to stall. They do mean the “best” exercise is often the one you can do safely, consistently, and without flaring up pain for the next two days.
For post-surgical seniors with arthritis, Ohio State’s PT education resource notes that aquatic therapy and carefully progressed interval work can be appropriate for some patients at the right stage of healing. That matches what we see in practice. Some people need pool-based exercise first because land walking is too irritating. Others need brief conditioning intervals later because strength alone is not enough to get them back to daily life.
Practical modifications often include:
- Reducing load: chair-supported exercises instead of unsupported standing work
- Changing surface: pool exercise or recumbent equipment when walking is too painful
- Shortening sessions: several brief exercise blocks instead of one longer workout
- Using higher supports: countertop, walker, cane, or rail while balance improves
The goal is not to force your body through a standard routine. The goal is to choose the version of each exercise that protects healing tissue, respects your other joint issues, and still gives you a reason to trust movement again.
Listening to Your Body and Overcoming Recovery Fears
A lot of people think the hard part of rehab is physical. Often the harder part is interpretation. You feel a pull, ache, twinge, or stiffness and immediately wonder if you’ve damaged something.
That uncertainty can make you either stop moving completely or push too aggressively to prove you’re okay. Neither response is very useful.
Red flags that mean stop and check in
Some symptoms are expected with exercise after operation. Mild soreness, temporary fatigue, and brief stiffness can be normal. Other signs deserve prompt medical guidance.
Stop exercising and contact your surgeon or rehab team if you notice:
- Sharp or escalating pain: especially if it doesn’t settle with rest
- Marked swelling or a sudden increase in swelling: especially when it’s new or clearly worse
- Drainage, redness, or heat around the incision: particularly if the wound appearance changes
- Shortness of breath, chest symptoms, or feeling unwell: treat these as urgent concerns
- Loss of function: if a movement that was manageable suddenly becomes much harder
Fear of movement is common, not a personal failure

After orthopedic procedures, this review of exercise after surgery reports that 40 to 60% of patients experience kinesiophobia, or fear of movement, and that this fear can delay recovery by 2 to 4 weeks. The same source notes that combining cognitive-behavioral strategies with physical therapy can reduce that fear by 35% and improve adherence by 50%.
That matters because fear changes behavior. It makes people hold their breath, stiffen up, skip exercises, and interpret every sensation as danger.
What helps in real life:
- Use micro-goals: “I’ll do one safe walk to the kitchen and back” is better than “I need to be normal again.”
- Separate discomfort from harm: stretching, muscle effort, and post-op stiffness don’t always mean injury.
- Track wins: note what improved, even if it’s small.
- Say the fear out loud: once a therapist hears it, they can often adjust the plan and explain what’s safe.
Confidence rarely appears before movement. It usually grows because of repeated safe movement.
When Professional Guidance is Your Best Next Step
A blog can give you a framework. It can help you understand why movement matters, what early exercises usually look like, and when to be cautious. What it can’t do is examine your incision, test your strength, watch your gait, or adjust your plan when a flare-up changes the picture.
That’s where individualized care becomes important. Recovery is rarely a straight line. Swelling changes. Pain shifts from day to day. Some people need more mobility work. Others need protection, balance training, scar mobility guidance, or a better return-to-walking strategy.
There’s also a strong reason not to treat the first month after discharge casually. Research in this study on postoperative physical activity and functional recovery found that patients who maintained higher levels of physical activity one month after discharge had significantly higher levels of physical functioning up to three months post-discharge. Guided consistency matters.
Professional rehab also helps connect exercise to the rest of recovery. Sleep, pacing, swelling management, footwear, home setup, and nutrition all influence how well you tolerate activity. If you’re trying to support healing with food choices as well, a tool like an AI nutritionist for personalized dietary advice may help you organize meal planning around your needs, especially when appetite and routine are off after surgery.
If you live in Deerfield Beach or nearby, working with a team that understands post-surgical rehab can make the process feel less uncertain and more practical. The right plan should fit your surgery, your body, your home routine, and your real goals, whether that’s walking comfortably, getting back to work, or feeling steady on your feet again.
If you want a personalized plan for exercise after operation, contact MedAmerica Rehab Center. Their team can evaluate your current stage of healing, review your precautions, and build a recovery program that matches your surgery, symptoms, and daily life so you can move forward safely and confidently.