Unlock Mobility: Range of Motion ROM Exercises
You notice it in ordinary moments first. Reaching into a cabinet feels tight. Turning your head while driving feels restricted. Bending to pull on socks makes your back complain before your day even starts.
That loss of motion is frustrating because it changes more than one movement. It affects how you sit, walk, lift, sleep, and recover from pain. The good news is that range of motion ROM exercises are one of the simplest and most useful ways to restore comfortable movement when they are matched to the right stage of healing.
In the clinic, we use ROM work for people with arthritis, sciatica, neck pain, shoulder stiffness, post-surgical knee recovery, and the general wear-and-tear stiffness that builds up when life gets busy. The key is not doing random stretches. The key is using the right type of movement, at the right time, with the right amount of effort.
Understanding Range of Motion and Why It Matters
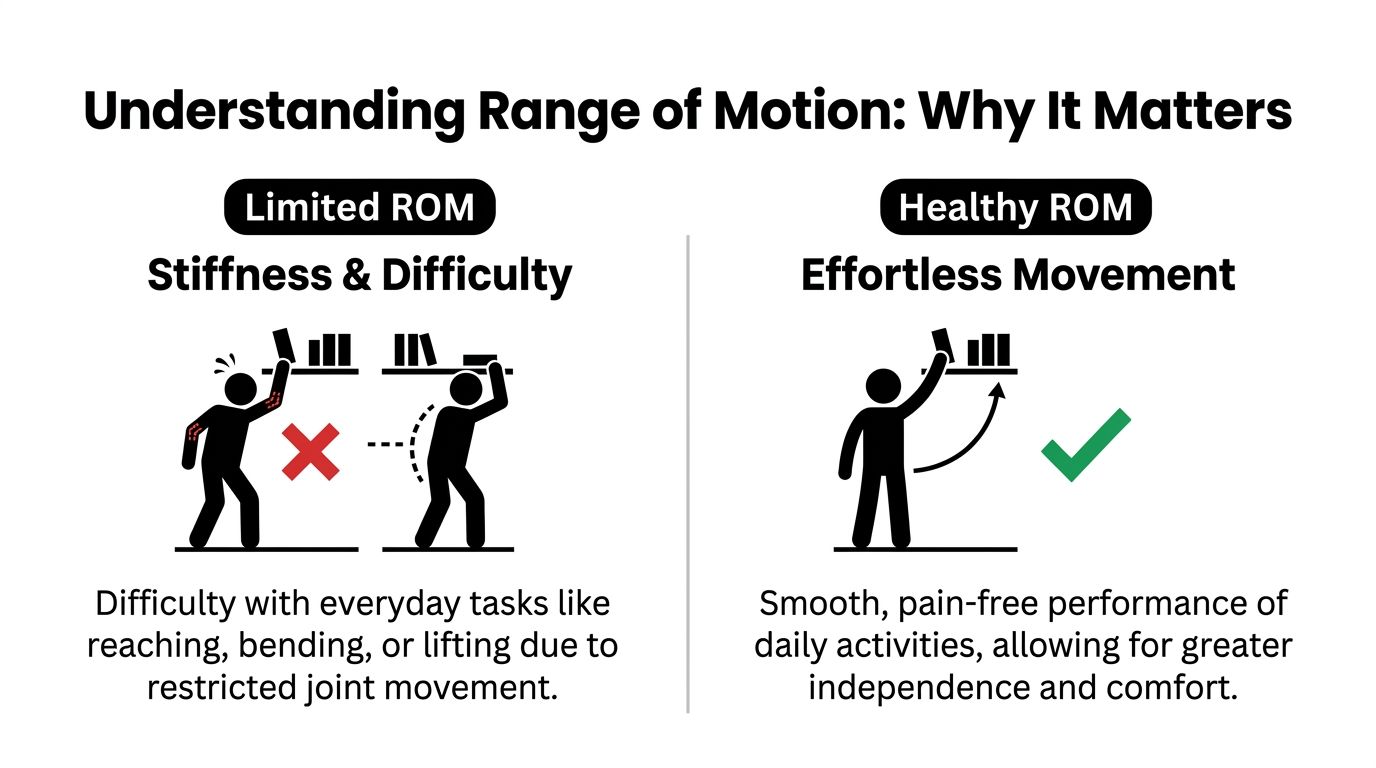
You feel the difference in small, practical ways. Reaching the seatbelt without twisting, turning to check a blind spot, or bending the knee enough to get in and out of a chair should not feel like a project. When a joint loses motion, the body starts compensating, and that often leads to more soreness, stiffness, and guarded movement.
Range of motion means how far a joint can move in the direction it is built to move. The shoulder lifts and rotates. The knee bends and straightens. The neck turns, nods, and tilts. Good ROM is not just about how far you can go. It is also about how smoothly and comfortably the joint moves during everyday tasks.
The three basic types of ROM
Physical therapists divide ROM work into passive, active-assistive, and active movement. The order matters because each one fits a different stage of healing.
Passive ROM means the joint is moved for you while your muscles stay relaxed. A therapist, caregiver, or device does the work. We often start here after surgery, during a pain flare, or any time the joint is too irritated or weak to move well on its own.
Active-assistive ROM means you help with the movement, but you are not doing all of it alone. Assistance might come from your other hand, a strap, a cane, or an over-the-door pulley exerciser for shoulder ROM. This stage is useful when motion is safe, but full muscular effort still causes strain, substitution, or pain.
Active ROM means you move the joint using your own muscles through the range you can control, building cleaner movement patterns, better coordination, and the strength needed to use that motion in real life.
In the clinic, progression is rarely automatic. We move from passive to active-assistive to active when the joint is calming down, swelling is manageable, and the movement quality is improving. If a patient can get farther only by hiking the shoulder, twisting the trunk, or holding their breath, the joint is not really ready for the next step yet.
Why therapists measure it
ROM should be measured, not guessed. Therapists compare the involved joint to expected motion and, when appropriate, to the other side. For example, a healthy knee typically flexes to a significant degree.
That number matters less than the function attached to it. A person may have enough knee motion to walk on level ground but still not enough to manage stairs comfortably. A shoulder may lift partway overhead but still fall short when reaching into a cabinet or washing hair.
This is also why we look at the quality of movement, not just the endpoint. Pain, stiffness, muscle guarding, and poor control can all limit ROM in different ways, and each one calls for a different treatment approach. If you want to understand how clinicians and digital tools accurately test range of motion, that overview gives helpful context on measuring movement in a more structured way.
Practical takeaway: ROM work helps restore the movement you need for daily life. The best results come from matching the type of ROM to the joint, the condition, and the stage of healing.
A Step-by-Step Guide to ROM Exercises for Major Joints
The safest home ROM routine looks controlled and almost boring. That is a good thing. Quick, jerky motion usually irritates tissue. Smooth motion usually helps it.
Start in a supported position. Sit tall or lie down comfortably. Breathe normally. Move only into a gentle stretch or mild pulling sensation, not sharp pain.

Neck movements
Neck ROM should feel easy and unforced. Keep your shoulders relaxed.
Chin nods
Sit upright. Gently tuck your chin as if making a small double chin. Return to neutral. This helps with the stiff, forward-head posture many people develop at desks.
Turn right and left
Rotate your head as if looking over one shoulder, then the other. Stop before pain or dizziness. You should feel a mild stretch, not a pinch.
Ear toward shoulder
Tilt your head toward one shoulder without lifting the shoulder. Come back to center and switch sides. This is often helpful when the upper trapezius feels tight.
What to avoid with the neck
- Fast circles: Full neck circles can bother some people with joint irritation.
- Forcing through headaches: If a movement triggers or worsens a headache, stop.
- Ignoring arm symptoms: Tingling, numbness, or shooting pain into the arm deserves attention.
Shoulder movements
Shoulders often stiffen after surgery, immobilization, or from guarding pain. The biggest mistake I see is shrugging the shoulder instead of moving the joint.
Pendulum
Lean forward with one hand on a table or counter for support. Let the other arm hang. Use your body to create small circles or forward-back motions. Keep the shoulder relaxed.
Table slides
Sit facing a table with a towel under your hand. Slide the hand forward as your trunk leans slightly, then return. This is a gentle way to restore overhead motion.
Wall climbs or finger walks
Face a wall and walk your fingers upward as far as comfortable, then come back down slowly. Keep the motion smooth. Do not arch your low back to fake extra reach.
Assisted overhead reach
Use your other hand, a cane, or a pulley to help lift the arm if active lifting is limited. For people who need a home tool for this stage, an over-the-door pulley exerciser is one common option for active-assistive shoulder work.
Elbow and forearm movements
Elbows and forearms get stiff quickly after splinting, fractures, tendon irritation, or overuse.
Elbow bend and straighten
Sit or stand tall. Bend the elbow fully, then straighten it as much as comfortable. Keep the upper arm close to your side.
Palm up and palm down
Bend your elbow to your side. Rotate the forearm so the palm faces up, then down. This motion is easy to lose after wrist or elbow problems.
Gentle end-range hold
If the elbow feels blocked, pause briefly at the end of the comfortable range, then come out of it. The pause should feel like a stretch, not a strain.
Wrist and hand movements
These are especially important for arthritis, desk work, and recovery after hand or forearm injury.
Wrist flex and extend
Rest your forearm on a table. Bend the wrist up, then down. Keep the fingers relaxed rather than clenched.
Open and close the hand
Spread the fingers wide, then make a gentle fist. This helps with morning hand stiffness.
Thumb to fingertip
Touch the thumb to each fingertip one at a time. This works well for dexterity and joint mobility.
Tip: If your hands are stiff in the morning, do these after a warm shower or after resting your hands in comfortably warm water.
A quick visual demonstration can help some people clean up their form before they build a routine at home.
Thoracic spine and trunk movements
Back stiffness is not always a low back problem. Many people need better movement through the mid-back and rib cage.
Seated trunk rotation
Sit upright with arms crossed over your chest. Turn gently to one side, then the other. Think of the ribs turning, not the knees shifting.
Side bend
Reach one hand down the side of your leg while the other side lengthens. Return to center and repeat on the other side.
Cat-camel
On hands and knees, round your back gently, then arch it gently. This is a mobility exercise, not a stretch contest.
Low back and pelvis movements
For the low back, smaller is often better at first.
Pelvic tilts
Lie on your back with knees bent. Flatten your lower back gently into the bed or floor, then relax. This is a simple way to wake up movement without a lot of strain.
Knee rocks
With both knees bent, let them move a short distance side to side. Keep the motion easy and controlled.
Single knee to chest
Bring one knee toward your chest with your hands behind the thigh or over the shin if comfortable. Return slowly. This often helps people who feel stiff after sitting.
Hip movements
Hip ROM affects your stride, balance, and ability to get in and out of chairs.
Heel slides
Lie on your back and slide one heel toward your body, bending the knee and hip together, then slide it back down.
Hip abduction
Lie on your back or stand with support. Move one leg out to the side, then return. Keep the pelvis level.
Hip rotation
Lying on your back with knees bent, let one knee roll slightly inward and outward within comfort. This can help with the feeling of hip tightness that shows up during turning or pivoting.
Knee movements
Knee motion matters for walking, stair climbing, sitting, and getting up from the toilet. People often focus on bending and forget that straightening is just as important.
Heel slides for knee flexion
Slide the heel toward your body until you feel a stretch in the front of the knee or thigh. Pause gently, then straighten.
Seated knee extension
Sit in a chair and slowly straighten one knee, then lower it. This is active ROM and also begins to wake up quadriceps control.
Supported knee extension stretch
Place the heel on a pillow or stool so the knee can relax downward into a straighter position. This should feel mild. Forcing extension can irritate the joint.
Ankle and foot movements
Ankles are easy to ignore until they stiffen and affect walking or balance.
Ankle pumps
Point the foot down, then pull the toes up toward you. This is especially helpful after long periods of sitting or lying down.
Ankle circles
Draw slow circles with the foot in both directions. Keep the rest of the leg relaxed.
Toe curls and spreads
Curl the toes, then spread them. Small joints matter for balance.
How the movement should feel
Use these simple rules at home:
- Mild stretch is acceptable: A pulling sensation is fine.
- Sharp pain is not: Stop if the motion feels stabbing, catching, or unstable.
- Motion should look controlled: If you have to twist, shrug, or hold your breath, reduce the range.
- The joint should calm down afterward: Temporary mild soreness can happen. Lasting irritation means you did too much.
A simple full-body sequence
If you want one easy flow on a stiff day, try this order:
- Neck turns and side tilts
- Shoulder table slides or wall climbs
- Seated trunk rotation
- Pelvic tilts
- Heel slides
- Ankle pumps
That sequence moves from top to bottom, warms the body gradually, and works well when you feel generally tight rather than dealing with one isolated joint.
Sample ROM Routines for Common Conditions
Many individuals do better with a short routine that matches their actual problem than with a long list of unrelated exercises. The right combination gives a joint movement without adding irritation.
Arthritis and morning stiffness
The common pattern is predictable. You wake up stiff, especially in the hands, knees, hips, or shoulders. The body usually loosens after you start moving, but the first part of the day feels slow and achy.
A simple arthritis-friendly routine starts with warmth and small motion:
- Hand open-close and thumb touches
- Shoulder table slides
- Seated trunk rotation
- Heel slides
- Ankle pumps
This works because arthritic joints usually respond better to frequent gentle movement than to one hard stretch. Many older adults also benefit from broader mobility exercises for seniors that support balance, joint motion, and confidence with daily activity.

Sciatica and low back guarding
People with sciatica often move less because they are afraid of provoking leg pain. That fear is understandable, but too much guarding usually makes the back and hips stiffer.
A starting routine often includes:
- Pelvic tilts
- Knee rocks
- Single knee to chest if tolerated
- Gentle hip abduction
- Ankle pumps if symptoms worsen with sitting
The purpose is not aggressive stretching of the nerve. The purpose is restoring calmer motion in the low back, pelvis, and hips so the body stops bracing every movement.
For some patients, unloading body weight in water makes early motion easier. Pool-based therapy can help people move with less guarding, and that is one reason some patients transition into physical therapy in a pool when land exercise feels too irritating.
Post-surgical knee recovery
For this, progression matters most. Right after surgery, the knee may be swollen, sore, and difficult to move. Early on, passive motion or assisted motion can be more realistic than forcing active bending.
For total knee replacement patients, Continuous Passive Motion or CPM can be used as a PROM tool. Studies show that 2-hour sessions, 2 to 3 times daily, starting at 0 to 40 degrees and progressing 5 to 10 degrees daily, can produce 20 to 30 percent greater ROM gains at 6 weeks than manual therapy alone (physio-pedia.com/Range_of_Motion).
A typical progression looks like this in practical terms:
Early phase
The knee gets gentle passive or assisted bending and straightening. Swelling control matters. Positioning matters. Pushing too hard too early usually backfires.
Middle phase
The patient begins helping more with heel slides, seated knee extension, and supported transfers. The goal is smoother motion and better confidence.
Later phase
The work shifts toward full active ROM, walking mechanics, stair work, and strength layered on top of restored motion.
Clinical reality: A knee that gets irritated after every session rarely improves as well as a knee that is challenged consistently and allowed to settle down between sessions.
Neck and shoulder desk stiffness
This group usually tells me the same thing. Pain builds during the day, then the shoulder and neck feel locked up by evening.
A practical routine is short:
- Chin nods
- Neck turns
- Shoulder rolls kept small and relaxed
- Wall climbs
- Forearm palm-up and palm-down rotation
These movements work because they address the areas that stiffen when the head stays forward and the arms live in front of the body for hours.
Optimizing Your ROM Program Dosage and Progression
A better ROM program is not the one that feels hardest. It is the one your joint will tolerate well enough to repeat tomorrow.
That is the part many patients miss. A shoulder, knee, or ankle usually improves faster with brief, repeatable practice than with one long session that leaves it sore, stiff, and protective for the rest of the day. In clinic, I look for the smallest dose that improves motion without stirring up a flare. Then I build from there.
A 2020 study found that flexibility gains in common ROM tests showed up early, with many improvements leveling off after the first few repetitions (pmc.ncbi.nlm.nih.gov/articles/PMC7728808). This finding supports a more efficient approach. Get the useful motion, then stop before technique slips or the joint starts guarding.
A practical dosage framework
Use this as a starting point. Then adjust based on irritability, swelling, fatigue, and how the joint feels later the same day.
| Goal | Frequency | Sets x Repetitions | Guidance |
|---|---|---|---|
| Maintain motion during stiffness or inactivity | At least twice daily | 1 set x 10 repetitions per motion | Use gentle, smooth movement. Stay well below pain. |
| Restore motion after injury or flare-up | Short, frequent sessions through the day | 1 to 2 sets, keeping most motions within the first few useful repetitions | Stop when motion becomes less smooth or symptoms increase. |
| Transition from assisted to active control | Daily | 1 to 2 sets of controlled repetitions | Reduce outside help gradually. Keep quality higher than range. |
| Build motion into functional tasks | Daily practice | Integrated into normal movement | Use the new motion during reaching, walking, dressing, and transfers. |
The twice-daily, 10-repetition guideline is a reasonable baseline for home practice. It works well for many people because it gives the joint regular input without turning each session into a strain test.
When to move from passive to active
Professional progression matters at this stage. The goal is not to stay with passive motion too long, but not to rush past it either.
Start with passive ROM when the joint is too painful, weak, swollen, or guarded to move well on its own. Move to active-assistive ROM when the joint can tolerate motion without a clear increase in pain, swelling, or muscle spasm during or after the session.
Then move to active ROM when these signs are present:
- You can initiate the motion yourself
- The movement stays controlled from start to finish
- Nearby body parts are not taking over
- Symptoms settle after practice instead of building over the day
I watch this closely in the clinic. A shoulder that shrugs toward the ear during elevation still needs better support and motor control. A knee that bends only by twisting the trunk is not ready for aggressive progression. Clean movement usually leads to more lasting gains than forcing extra degrees with compensation.
How to progress without irritating the joint
Progress one variable at a time. Increase range a little, or add a few repetitions, or reduce assistance. Do not change everything at once.
A simple rule works well. If motion improves during the session and returns to baseline or better afterward, the dose was probably appropriate. If the joint becomes hotter, more swollen, more painful, or harder to move for hours afterward, the dose was too high.
In practice, joints often respond better to short, frequent sessions, unlike a single long session that can leave you sore and guarded.
What usually works and what usually does not
Works well
- Gentle repetitions done consistently
- Several short sessions across the day
- Pairing ROM work with steady breathing and relaxed muscles
- Progressing only after the joint calms down reliably at the current level
Usually fails
- Occasional marathon stretching sessions
- Forcing painful end range
- Chasing numbers while movement quality gets worse
- Adding strengthening before the joint has enough basic motion to move cleanly
Best rule for home practice: Leave the joint a little better, not a lot angrier.
Precautions and When to See a Physical Therapist
ROM exercises are safe for many people, but not every painful joint should be pushed. Some situations need modification, and some need an evaluation before you continue.
Know the difference between stretch discomfort and warning pain
A gentle stretch, mild pulling, or light stiffness as you move is usually acceptable. That is common when a joint has been inactive.
Sharp pain, catching, sudden pinching, strong throbbing, or a feeling that the joint is slipping is different. Stop the motion if you feel that.

Be careful in these situations
Do not treat every stiff joint the same. Use extra caution if you have:
- A recent fracture or suspected fracture
- A recent surgery with movement restrictions
- An infection or unexplained redness and heat
- A joint that feels unstable
- Severe swelling that is getting worse
- New numbness, tingling, or weakness
- Dizziness with neck movement
These are not “push through it” situations.
Red flags that mean stop and get help
Call a physical therapist or your physician if you notice:
- A sudden loss of motion
- Pain that keeps increasing during or after exercise
- New swelling that does not settle
- Pain shooting down an arm or leg
- Difficulty bearing weight
- A joint that locks or gives way
People often wait too long because they assume stiffness will pass on its own. Sometimes it does. Sometimes the body starts building bad movement habits around the pain, and those habits are harder to unwind later.
Getting guidance early is not overreacting. It is efficient. A therapist can tell you whether you need passive work, active-assistive work, or a more advanced routine, and can also catch the compensation patterns that slow recovery.
Start Moving Better Today in Deerfield Beach
Many do not need a complicated plan to begin. They need a smart one. Gentle, regular movement often does more for pain and daily function than occasional hard stretching sessions.
If your shoulder feels stuck, your knee does not bend well after surgery, your neck is tight from desk work, or your back stiffens every morning, consistent range of motion ROM exercises can help restore movement that feels normal again. The key is matching the exercise type to your stage of healing, then progressing from passive to active only when your body is ready.
If you live nearby and want a plan built around your pain, your surgery, or your goals, local care matters. At MedAmerica, we work with adults, seniors, post-surgical patients, athletes, and injury patients who need a practical path forward, not generic advice. If you are looking for physical therapy in Deerfield Beach, a guided ROM program can give you a clear starting point and a safer progression.
You do not have to guess whether you are doing too much, too little, or the wrong type of movement. The right plan should help you move better in real life, not just during exercise.
If pain, stiffness, or post-surgical limitation is keeping you from moving comfortably, contact MedAmerica Rehab Center. Our team can evaluate your joint motion, identify what is limiting you, and build a personalized program that fits your condition and daily life.