Hand Physical Therapy for Pain Relief & Function
Your hand usually gets your attention only when it stops cooperating.
A coffee mug feels heavier than it should. Turning a key sends a sharp reminder into your wrist. You start using your other hand to open jars, button a shirt, zip a bag, or hold your phone. Even typing a short email becomes something you brace for instead of something you do without thinking.
That is the part many people find unsettling. Hand pain does not just hurt. It interrupts independence. It slows work, chores, exercise, driving, cooking, grooming, sleep, and the small routines that make a day feel normal.
Hand physical therapy is built for that exact problem. It is not a random set of stretches or a generic rehab sheet. It is a structured plan to reduce pain, protect healing tissue, restore motion, rebuild strength, and help you trust your hand again in tasks.
Patients often come in worried that they waited too long, or that the only options left are to live with it or consider surgery. In many cases, neither is true. The hand responds well to precise treatment when the plan matches the diagnosis, the stage of healing, and the demands of daily life.
Regaining Control When Hand Pain Disrupts Your Life
A hand problem rarely announces itself with one dramatic moment. Sometimes it starts with a fingertip that catches when you make a fist. Sometimes it is numbness while driving. Sometimes it is a wrist that aches after a long day at the computer or a thumb that protests every time you grip a pan.
Then the workarounds begin.
You stop carrying grocery bags with one hand. You use your forearm to push open doors. You avoid hobbies that used to clear your mind, like gardening, golf, sewing, weight training, or playing an instrument. If the problem is in your dominant hand, the frustration builds faster because every simple task suddenly asks for planning.
Daily life is where hand problems become real
In the clinic, the most useful question is often not “Where does it hurt?” It is “What can’t you do comfortably anymore?”
That answer tells us much more than a pain rating alone. A retired patient may want to grip the rail confidently and cook without dropping dishes. An office worker may need to type, text, and use a mouse all day. A mechanic, hairstylist, nurse, server, or carpenter may need repeated pinch, grip, lifting, twisting, and fine motor control.
Those details shape treatment.
Key takeaway: Good hand physical therapy targets the job your hand needs to do, not just the body part that hurts.
Recovery works best when it is specific
The hand is small, but the problems are not simple. Pain can come from irritated tendons, a compressed nerve, stiff joints, post-surgical scar tissue, swelling, weakness, overuse, or a healing fracture. Two people can say “my wrist hurts” and need completely different plans.
That is why hand physical therapy works best as a partnership. The therapist measures what is limited, identifies what is driving the problem, and builds a plan you can follow in the clinic and at home. The patient brings the other half by showing up consistently and doing the right amount of work, not too little and not too much.
The good news is that progress is usually noticeable in meaningful ways. You may sleep better first. Then turning a doorknob becomes easier. Then your grip steadies. Then you stop thinking about every movement.
That return of confidence matters as much as pain relief.
Understanding Hand Physical Therapy and Your Therapist
Your hand works like a compact machine with many moving parts packed into a small space. Joints have to glide. Tendons have to slide. Nerves have to move and signal properly. Muscles have to coordinate timing and force. If one part gets stiff, irritated, weak, or compressed, the whole system changes its behavior.
That is why hand physical therapy is a specialty.

Why specialization matters
A general rehabilitation program can help broad mobility and strength problems. Hand rehabilitation often needs more precision.
A stiff finger after tendon repair is not treated the same way as thumb arthritis. Numbness from carpal tunnel behaves differently from pain caused by tendon irritation. A splint that helps one condition can aggravate another if it is worn at the wrong time or fitted poorly.
That precision is one reason the field developed its own advanced training standards. Certified Hand Therapists need a minimum of 3 years of clinical experience and 4,000 hours or more in direct hand and upper extremity practice before passing a rigorous certification exam, according to this overview of hand therapy training and workplace injury relevance from Pro Staff Physical Therapy. The same source notes that hand and finger injuries account for 23% of all work-related injuries in the U.S.
That combination matters to patients. You are not just seeing someone who understands exercise. You are seeing someone trained to sort out subtle motion loss, tendon mechanics, nerve symptoms, edema, scar behavior, orthotic needs, and return-to-function planning.
What a hand therapist does
A hand therapist does more than guide exercise.
They measure motion in specific joints. They evaluate tendon glide, pinch patterns, swelling, sensation, coordination, and functional use. They decide when tissue needs protection and when it needs motion. They may fabricate or adjust custom orthoses, teach activity modification, and coordinate care with the physician when post-surgical precautions matter.
For some patients, a broader rehab overview is also helpful, especially if symptoms affect the arm, shoulder, neck, posture, or overall mobility. If you want context on general physical therapy services, that resource gives a useful big-picture summary of how physical therapy supports movement and pain relief across many conditions.
Hand therapy and occupational therapy often overlap
Many patients are surprised to learn that upper extremity rehab often blends principles from physical therapy and occupational therapy. That overlap is practical. Hand problems affect motion and strength, but they also affect dressing, grooming, writing, lifting, cooking, and work tasks.
If you want to understand that side of care more clearly, this overview of occupational therapy is a helpful reference.
Practical tip: The best therapist for a hand problem is not just someone who knows anatomy. It is someone who can connect anatomy to the exact task you need to do again.
The patient role is active
Specialized care does not mean passive care.
Even the best treatment in the clinic cannot replace the daily choices that shape healing. Wearing the splint as prescribed, pacing hand use, following exercise timing, and avoiding the “it feels better so I did everything at once” mistake often determines whether progress stays smooth or stalls.
Good hand physical therapy gives you a map. Good results come from following it closely.
Common Conditions We Treat and Your Recovery Goals
Hand symptoms can feel random to the patient. To a therapist, patterns matter. Pain location, numbness, stiffness, clicking, swelling, weakness, and task intolerance usually point toward a smaller set of likely problems.
That matters because hand physical therapy is most effective when the treatment matches the condition and the recovery target. The target is not just “less pain.” It is a useful return to daily life.
Research reviewed across 475 studies found that orthopedic issues of the upper extremity have a global prevalence of 26.9%. For osteoarthritis, exercise appeared in 74% of studies and manual techniques in 44%. For tendon injuries, orthotics were used in 77% of cases and exercise in 81%, showing how established the main treatment pathways are for these diagnoses in hand therapy research, as summarized in the review at the National Library of Medicine.
Common Hand Conditions and Therapy Goals
| Condition | Common Symptoms | Primary Therapy Goals |
|---|---|---|
| Carpal tunnel syndrome | Numbness, tingling, hand fatigue, night symptoms, dropping objects | Reduce nerve irritation, improve tendon and nerve mobility, restore grip confidence, make typing, driving, and sleep more comfortable |
| Osteoarthritis of the hand or thumb | Aching, stiffness, swelling, weak pinch, pain with opening jars or turning lids | Improve joint motion where possible, reduce strain on irritated joints, support pinch tasks, protect function in cooking, dressing, writing, and household tasks |
| Trigger finger | Catching, locking, painful gripping, finger stiffness in the morning | Calm tendon irritation, improve smooth finger motion, reduce painful catching, restore comfortable grasp and release |
| Tendon injuries or repairs | Pain, weakness, stiffness, limited finger bend or straightening, scar sensitivity | Protect healing tissue, restore tendon glide, improve range of motion, rebuild grip and pinch for daily tasks |
| Fractures and post-immobilization stiffness | Swelling, pain, limited joint motion, weakness after cast or brace removal | Recover mobility safely, reduce swelling, improve hand use, return to lifting, carrying, and fine motor activity |
| Wrist sprains and overuse injuries | Pain with weight bearing, gripping, twisting, or repetitive use | Reduce irritation, restore stability and motion, improve load tolerance for work, exercise, and chores |
| Arthritis-related hand weakness in seniors | Stiffness, reduced grip, trouble holding rails, utensils, or small items | Preserve safe hand function, improve confidence with support surfaces, support independence and reduce the effect of weakness on balance |
Matching the goal to real life
A useful plan starts with functional goals that matter to the patient.
That may include:
- Work tasks: gripping tools, using a keyboard, handling trays, lifting materials, writing, or operating machinery
- Home tasks: cooking, cleaning, opening containers, carrying laundry, bathing, fastening clothing
- Recreation: tennis, golf, pickleball, yoga, weight training, crafts, gardening, piano, fishing
- Safety and independence: using a cane or walker safely, holding stair rails, steadying yourself during transfers
Some conditions improve by unloading irritated tissue first. Others improve only when we start controlled movement early. That difference is one reason online advice can be hit or miss. A hand that needs protection can get worse from aggressive stretching. A hand that needs motion can stiffen further if the patient keeps “resting” it for too long.
For readers dealing specifically with numbness, tingling, and grip weakness, this page on carpal tunnel gives a condition-specific overview.
What works: Clear diagnosis, specific activity goals, and the right balance between protection and movement.
What does not: Treating every hand problem like inflammation alone, or every stiff hand as if it needs more stretching.
What to Expect During Your First Hand Therapy Evaluation
The first visit is not a workout. It is a problem-solving session.
Many patients feel better once they see how detailed the evaluation is, because the process shows that treatment is being built around their hand, not pulled from a standard template. If your symptoms have been frustrating or inconsistent, this first appointment often gives the first real explanation of what is happening.
The conversation matters more than people expect
The evaluation starts with history.
You will usually be asked when symptoms began, what movements aggravate them, whether symptoms are constant or intermittent, whether you have had surgery or imaging, and what your day looks like. Repetitive gripping at work, long hours on a laptop, lifting a grandchild, using a walker, playing racquet sports, or sleeping with a bent wrist can all change the clinical picture.
Your goals belong in that conversation too. “I want to get back to the gym” is useful. “I want to hold a frying pan, fasten my bra, and sleep without numbness” is even better because it gives the therapist functional targets.
The physical exam is precise
A hand evaluation usually includes observation first. We compare both sides. We look at posture, swelling, color, scar mobility, protective guarding, and whether a finger or thumb moves differently from the others.
Then we measure.
A key metric in hand rehabilitation is Total Active Motion, or TAM, which tracks a digit’s functional movement. Therapists use goniometers for joint range of motion and dynamometers for pinch strength. Thumb opposition can be graded on the 10-point Kapandji scale, which gives precise baseline data and a way to document recovery, as outlined in this hand evaluation guide from Hand Therapy Academy.
Common parts of the exam
- Range of motion testing: This shows whether the problem is stiffness, weakness, pain inhibition, swelling, or a combination.
- Strength testing: Grip and pinch patterns help identify what is limited and what tasks are likely to be difficult.
- Sensation screening: Numbness and tingling are mapped carefully, especially when nerve compression or post-traumatic changes are suspected.
- Functional testing: We may ask about buttons, key pinch, lifting, writing, reaching into pockets, or simulated work tasks.
Tip: Bring your brace, splint, operative note, or imaging report if you have them. Those details can sharpen the plan quickly.
The plan starts at the first visit
Patients often expect to “get evaluated” and wait for a plan later. In good hand physical therapy, planning starts immediately.
You should leave understanding what structure appears irritated or stiff, what needs protection, what should start moving, what activities to modify, and what home work matters most right now. In some cases the first step is calm and protective. In others, the first step is early motion to prevent avoidable stiffness.
The purpose of all that measuring is simple. If we know exactly where you started, we can show real progress instead of guessing.
Your Personalized Toolkit of Evidence-Based Treatments
Many people think hand therapy means squeezing putty and doing finger stretches. Those are tools, but they are only a small part of the full treatment picture.
Good hand physical therapy combines timing, dosage, tissue protection, pain control, and progressive loading. The plan changes as your hand changes. Early on, the priority may be calming pain and protecting healing tissue. Later, the priority may be tendon glide, grip strength, work tolerance, or dexterity.
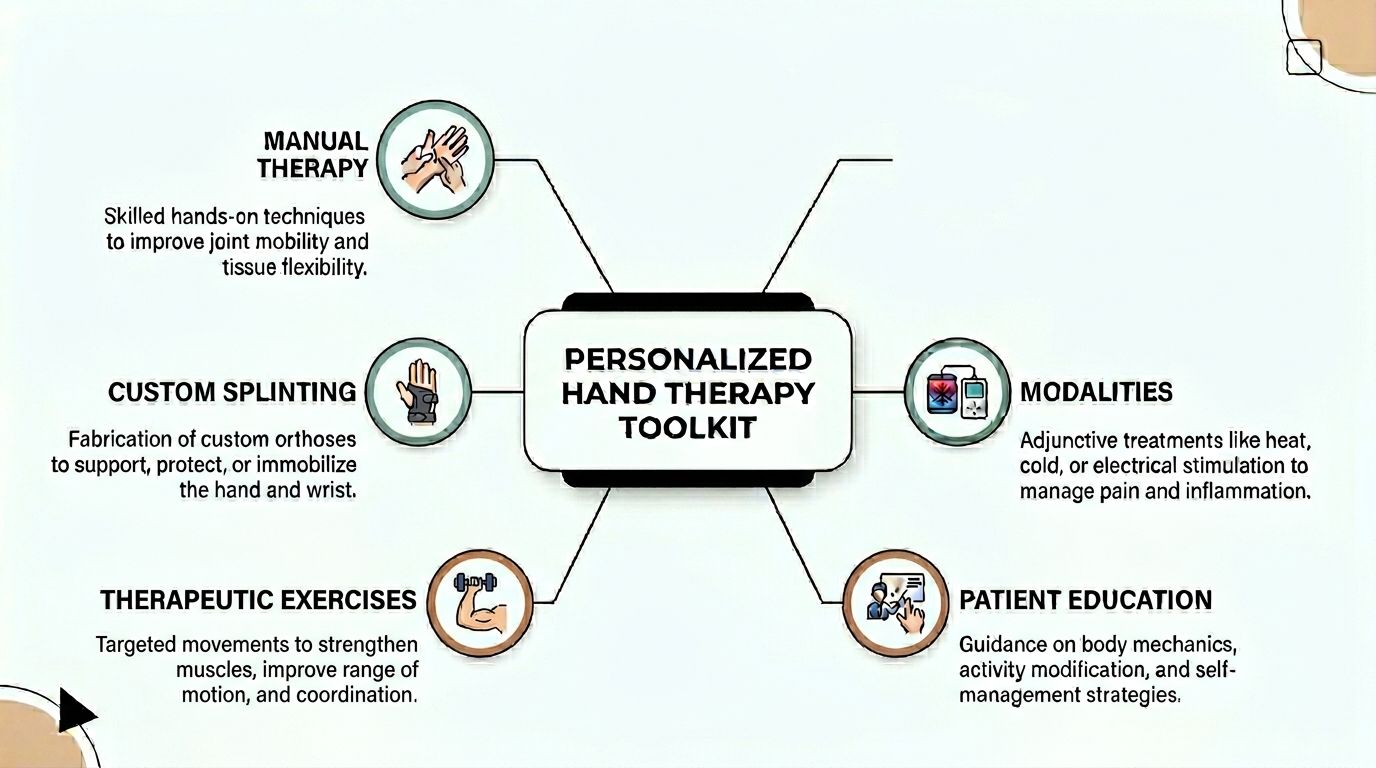
Manual therapy
Manual therapy is skilled hands-on treatment, not generic rubbing.
A therapist may mobilize stiff joints, work on scar mobility, reduce soft tissue restriction, or guide controlled movement that the patient cannot yet perform smoothly alone. The point is to improve mechanics. A finger joint that is not gliding well, or scar tissue that is tethering tendon movement, often needs more than simple home exercise.
Manual work also helps therapists feel tissue behavior directly. We can tell whether something is guarded, swollen, hypersensitive, or maturing well.
Therapeutic exercise
Exercise is where movement gets reclaimed and then made useful again.
Early exercise may look modest. Tendon glides. Joint blocking. Gentle opposition. Controlled wrist motion. It can feel almost too simple. That is often a good sign. Early rehab is about precision, not heroics.
Later exercise becomes more demanding:
- Mobility work: restoring finger bend, straightening, wrist motion, and thumb reach
- Strength work: putty, bands, pinch tasks, grip drills, resisted forearm work
- Coordination work: object manipulation, in-hand translation, dexterity tasks, task-specific retraining
- Functional loading: carrying, lifting, pushing, pulling, twisting, and work simulation
Custom splinting and orthoses
Custom splinting is one of the most useful parts of hand therapy because it solves a common rehab problem. Tissue may need protection and movement at the same time.
A custom orthosis can rest an irritated structure, guide a joint toward better positioning, protect a repair, or allow controlled motion while reducing strain. That is much different from buying a one-size-fits-all brace and hoping it is close enough.
Evidence from a hand therapy EMR and outcomes review notes that early controlled motion protocols using custom orthoses produce 85% to 90% excellent or good outcomes in flexor tendon repairs compared with 60% to 70% for older static splinting methods. The same source notes targeted exercises can rebuild grip strength to 90% of normal within 6 to 12 weeks in appropriate cases. Those figures appear in this summary of hand therapy documentation and treatment features from Proactive Chart.
That does not mean every patient needs aggressive early movement. It means the right orthosis can support the right movement at the right time.
Modalities and adjunctive care
Modalities can help when they are used for a clear purpose.
Heat may prepare stiff tissue for motion. Ice may calm an irritated area after loading. Electrical stimulation may support specific goals in selected cases. Ultrasound and other clinic-based modalities can be useful as part of a broader plan, not as stand-alone care.
In a multidisciplinary setting, some patients also benefit from adjunctive services such as shockwave therapy for stubborn soft tissue pain or acupuncture when pain sensitivity and muscle guarding remain high. Those additions do not replace exercise, splinting, or skilled progression. They can make those core treatments easier to tolerate and more effective when used thoughtfully.
For patients wondering when cold therapy fits into a rehab plan, this guide on an ice pack in physical therapy offers practical context.
Education changes outcomes
The best treatment plan fails if the patient overloads the hand between visits.
Education often sounds basic, but it is where many recoveries either stay on track or go sideways. Patients need to know how to lift differently, how long to wear a brace, when soreness is acceptable, what swelling means, how to use the non-dominant hand strategically, and when to stop “testing” the injured area every hour.
Clinical reality: More is not always better. Tissues heal with the right amount of stress. Too little slows recovery. Too much can restart irritation.
The strongest hand therapy plans use each tool for a reason. Manual work improves the motion available. Exercise teaches the body to use that motion. Splinting protects gains or protects healing tissue. Modalities reduce barriers. Education keeps progress from being undone at home.
Home Exercises and Realistic Timelines for Your Recovery
Clinic visits matter. Home practice is where momentum builds.
The hand learns through repetition, but it also gets irritated by repetition when the dose is wrong. The trick is doing the right movement often enough to help, without turning exercise into another source of inflammation. That is why home programs should feel specific and manageable, not like a second full-time job.

Examples of useful home work
A few common hand exercises show how this works.
Tendon glides help fingers move through different positions so the tendons slide rather than stick. These are often useful after stiffness, swelling, or surgery when the hand feels tight and clumsy.
Thumb opposition drills train the thumb to meet each fingertip with control. That matters for buttons, zippers, writing, keys, and pinch tasks.
Therapy putty or a soft resistance ball can rebuild grip and pinch gradually. At the right stage, this helps the hand tolerate daily loads again.
Wrist motion drills are often used after immobilization or overuse, especially when the wrist has become guarded and stiff.
What matters most is sequencing. A patient with an irritated tendon may need gentle glide work before strengthening. A patient who is very weak after immobilization may need motion work, then light loading, then task-based resistance.
Progression matters more than intensity
Many setbacks come from doing advanced work too soon.
A useful progression usually looks like this:
- Protect and calm: reduce irritation, manage swelling, restore comfortable basic motion.
- Move well: improve tendon glide, joint motion, and coordination.
- Load gradually: add resistance, gripping, pinching, and sustained use.
- Return to real tasks: work duties, household lifting, sports, hobbies, and balance-related hand use.
This short video can help you visualize how guided hand exercise fits into recovery.
Timelines should be realistic
Patients usually want one answer to “How long will this take?” Real recovery depends on the diagnosis, tissue healing stage, swelling, job demands, home consistency, and whether surgery occurred.
Still, some patterns are predictable. Early changes often show up first as less night pain, less swelling, or better ease with light tasks. Strength and endurance usually take longer than pain relief. Fine motor confidence often returns after mobility improves, not before.
If a plan includes splinting, manual therapy, exercise progression, and good home follow-through, the hand usually improves in layers. First comfort. Then motion. Then strength. Then tolerance for longer or heavier use.
Hand health affects balance in seniors
This is one connection many patients have never been told about.
Hand weakness is linked to a 15% higher fall risk in seniors, and the quadriga effect means stiffness in one digit can affect the grip and function of the whole hand, according to this summary on hand exercise considerations from Physiopedia. That matters when an older adult relies on rails, a cane, a walker, or a countertop for steadying.
A weaker, stiffer hand is not only a hand problem. It can become a balance and safety problem.
What works for seniors
For older adults, hand physical therapy should connect hand strength with whole-body safety.
- Grip with purpose: practice holding rails, cups, utensils, handles, and mobility devices safely
- Thumb and finger control: improve object handling so daily tasks require less compensation
- Combined balance training: pair hand use with sit-to-stand, stepping, transfers, and gait activities when appropriate
- Joint protection: reduce strain in arthritic hands so the patient can keep using the hand instead of avoiding it
Important: Pain that spikes for hours after home exercise usually means the dose is too high. Mild effort is useful. Flare-ups are not a badge of progress.
Consistency beats intensity. Five well-chosen minutes done regularly usually helps more than one long, aggressive session that leaves the hand angry for the rest of the day.
Begin Your Recovery at MedAmerica Rehab in Deerfield Beach
If your hand pain is changing how you work, sleep, drive, cook, train, or steady yourself, it is time to stop guessing.
The right time to start hand physical therapy is usually earlier than people think. Waiting often teaches the body compensation patterns that are harder to unwind later. Patients begin gripping differently, avoiding finger motion, overusing the opposite hand, or protecting the wrist so much that stiffness becomes a second problem layered on top of the first.
Signs it is worth scheduling
Consider an evaluation if you notice any of the following:
- Pain during ordinary tasks: opening containers, typing, lifting bags, grooming, fastening clothes
- Numbness or tingling: especially at night, while driving, or during repetitive hand use
- Lingering stiffness or weakness: after a fracture, surgery, sprain, or immobilization
- Loss of confidence: dropping items, avoiding grip, struggling with rails or support surfaces
Why a multidisciplinary clinic helps
Hand symptoms do not always stay isolated to the hand.
Wrist mechanics, forearm tension, shoulder position, neck irritation, postural habits, pain sensitivity, and whole-body balance can all influence recovery. That is one reason a multidisciplinary clinic can be helpful. A patient may need skilled hand rehab as the core plan, with selected support from acupuncture for pain control, chiropractic care when related mechanics contribute, or shockwave therapy when stubborn soft tissue pain limits progress.
This broader model is one reason patients often compare different Physical Therapy Clinics before choosing care. Looking at how clinics coordinate services, document progress, and match treatment to function is often more useful than judging a clinic by equipment alone.

Make the first step easy
A good clinic should make logistics simple, not confusing. Patients should be able to ask practical questions about appointments, insurance, documentation, and next steps without feeling lost in the process.
The most important thing is not having every answer before you call. It is getting the hand evaluated before a manageable problem becomes a longer recovery. Pain relief matters, but function matters just as much. The objective is to use your hand naturally again without planning your day around it.
If hand pain, stiffness, numbness, or weakness is interfering with your routine, schedule an evaluation with MedAmerica Rehab Center. Their Deerfield Beach team provides patient-centered hand and upper extremity care with physical therapy, chiropractic, acupuncture, and advanced shockwave therapy, so you can get a practical treatment plan that fits your condition, goals, and daily life.